

Copyrights: Yousef Veisani, Ali Delpisheh, Salman Khazaei, 2017. License: This work is licensed under a Creative Commons Attribution 4.0 International License.
Abstract
Tuberculosis (TB) has the second highest death rate in the world among infectious diseases after HIV/AIDS (Wei et al., 2016). TB epidemic is more important than it was supposed to be (Raviglione and Sulis, 2016). In 2015, 10.4 million new cases were occurred worldwide, among these, 5.9 million (56%) were male, 3.5 million (34%) were female, and 1.0 million (10%) of them was the child. It should be noted that 1.2 million (11%) of all new TB cases were occurred in people that living with HIV (PWLH). Although tuberculosis deaths are declined by about 22% between 2000 to 2015, still is remained among top 10 causes of death in 2015 (Uplekar et al., 2015; WHO, 2016).
Letter
Tuberculosis (TB) has the second highest death rate in the world among infectious diseases after HIV/AIDS (Wei et al., 2016). TB epidemic is more important than it was supposed to be Raviglione and Sulis, 2016. In 2015, 10.4 million new cases were occurred worldwide, among these, 5.9 million (56%) were male, 3.5 million (34%) were female, and 1.0 million (10%) of them was the child.
It should be noted that 1.2 million (11%) of all new TB cases were occurred in people that living with HIV (PWLH). Although tuberculosis deaths are declined by about 22% between 2000 to 2015, still is remained among top 10 causes of death in 2015 Uplekar et al., 2015WHO, 2016.
The three indicators for the End TB Strategy was conducted by the United Nations in 2015; percent of the reduction in some TB deaths, percent of the reduction in TB incidence rate, and percent of TB-affected families facing catastrophic costs due to TB. Indicators were targeted for the years 2030 and 2035, by milestones in 2020 and 2025, respectively Lönnroth and Raviglione, 2016Uplekar et al., 2015WHO, 2016 ( Table 1 ).
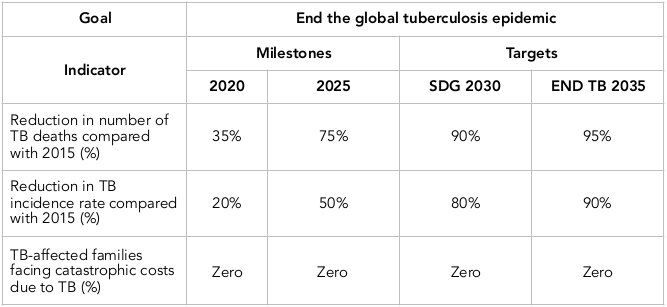
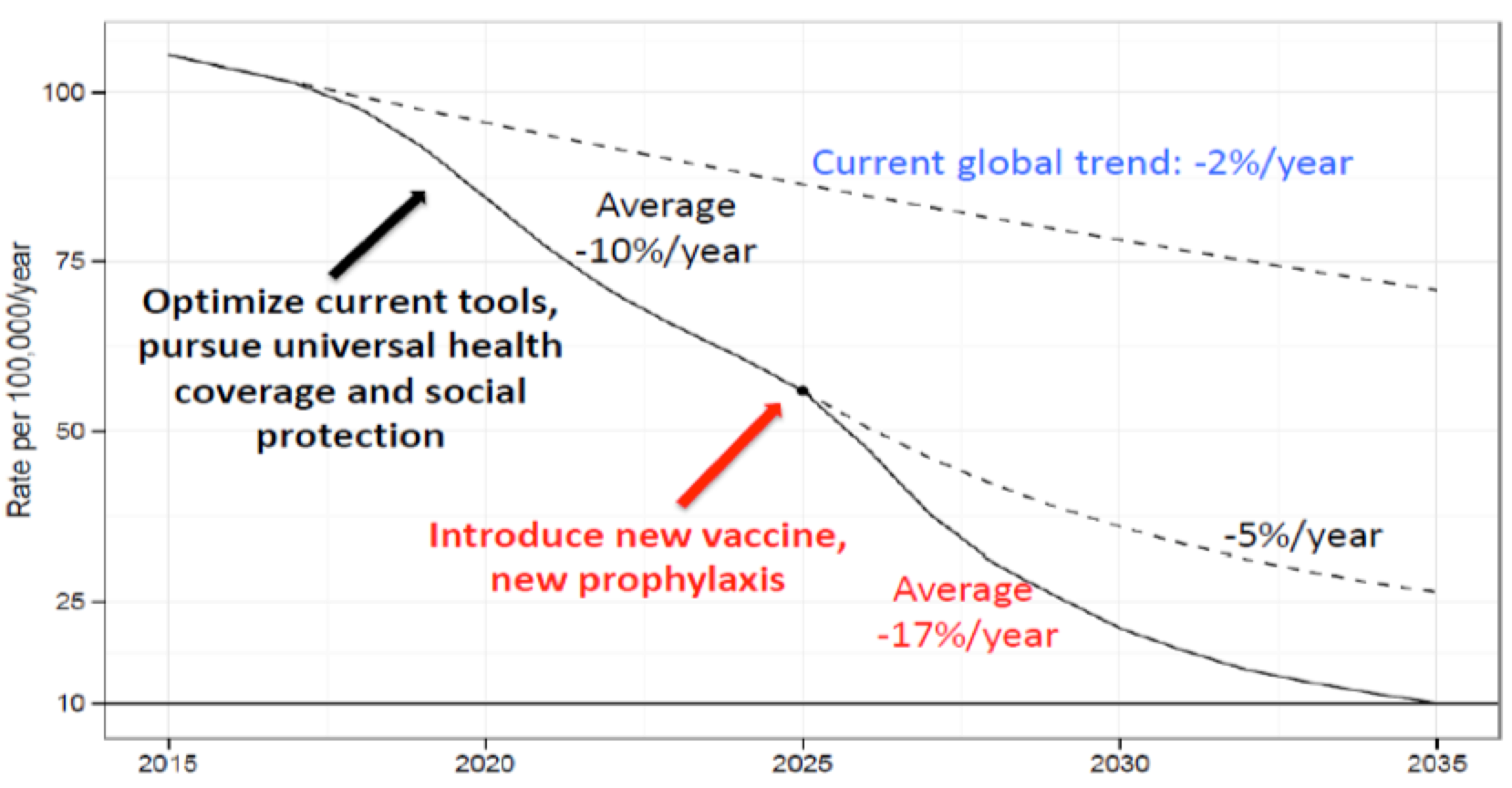
To achieve these targets, the annual TB incidence rates should be reduced to 10% per year by 2025 (from 2% per year in 2015). In second, the case-fatality ratio must be decline to 6.5% by 2025 (from 15% in 2015). As projected to maintain progress after millstone time and achieve the Sustainable Development Goals (SDGs) for 2030 and End TB 2035 targets new tools should be available in 2025 that compromise a new vaccine, conduct a new diagnostic approach, and more effective treatment for TB disease Taghizade Moghaddam et al., 2016WHO, 2016 ( Figure 1 ).
It is apparently detectable that failure in achieving to SDGs for 2030 and End TB 2035 targets will take severe concerns in both individual and global public health outcomes Dirlikov et al., 2015Lönnroth and Raviglione, 2016. WHO recommended implications for TB preventions such as encouraging the private sector to participate in TB care especially in low-income countries, documenting and evaluating social protection and economic support for TB patients in low-and middle income countries to assess of impact and sustainability, conducts of national surveys to assess of improve services to TB patient, beside these ending TB in world links to ending risk factors of poverty, such as non-communicable disease prevention, food security, and housing Lönnroth and Raviglione, 2016.
In finally above prevention strategies must be accompanied by priorities action plan for global progress towards TB and achieve to SDGs for 2030 and End TB 2035. Priorities action plan are following; identify undiagnosed cases (3 million not in TB care), MDR-TB crisis plan to deal with, appropriate and prompt treatment of TB/HIV cases, increase financing support at national level, and support innovation in the field of TB Cousins, 2016WHO, 2016.
Abbreviation
Tuberculosis (TB)
Sustainable Development Goals (SDGs)
World Health Organization (WHO)
Author contribution
All authors contributed in manuscript preparation. Veisani,Y and Khazaei,S obtained data and analyzed it. Delpisheh, A interpreted of data analysis. All authors drafted the first version and approve the final draft.
References
-
S.
Cousins.
Funding shortfalls put target to end TB epidemic by 2035 at risk. BMJ.
2016;
355
.
-
E.
Dirlikov,
M.
Raviglione,
F.
Scano.
Global tuberculosis control: Toward the 2015 targets and beyond. Annals of Internal Medicine.
2015;
163
:
52-58
.
-
K.
Lönnroth,
M.
Raviglione.
The WHO's new End TB Strategy in the post-2015 era of the Sustainable Development Goals. Transactions of the Royal Society of Tropical Medicine and Hygiene.
2016;
110
:
148-150
.
-
M.
Raviglione,
G.
Sulis.
Tuberculosis 2015: Burden, Challenges and Strategy for Control and Elimination. Infectious Disease Reports.
2016;
8
:
6570
.
-
H.
Taghizade Moghaddam,
Z.
Emami Moghadam,
G.
Khademi,
A.
Bahreini,
M.
Saeidi.
Tuberculosis: Past, Present and Future. International Journal of Pediatrics.
2016;
4
:
1243-1254
.
-
M.
Uplekar,
D.
Weil,
K.
Lonnroth,
E.
Jaramillo,
C.
Lienhardt,
H.M.
Dias,
D.
Falzon,
K.
Floyd,
G.
Gargioni,
H.
Getahun.
WHO's new End TB Strategy. The Lancet.
2015;
385
:
1799-1801
.
-
W.
Wei,
Z.
Wei-Sheng,
A.
Ahan,
Y.
Ci,
Z.
Wei-Wen,
C.
Ming-Qin.
The Characteristics of TB Epidemic and TB/HIV Co-Infection Epidemic: A 2007-2013 Retrospective Study in Urumqi, Xinjiang Province, China. PLOS ONE.
2016;
11
:
e0164947
.
-
WHO.
Global Tuberculosis Report. 2016
.
Comments
Downloads
Article Details
Volume & Issue : Vol 4 No 08 (2017)
Page No.: 1498-1501
Published on: 2017-08-14
Citations
Copyrights & License
This work is licensed under a Creative Commons Attribution 4.0 International License.
Search Panel
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Search for this article in:
Google Scholar
Researchgate
- HTML viewed - 5073 times
- Download PDF downloaded - 2312 times
- View Article downloaded - 14 times

{kind=link}
{kind=link}