

Copyrights: Farshad Rahimi, Masoud Sadeghi, Hamid Reza Mozaffari, 2017. License: This work is licensed under a Creative Commons Attribution 4.0 International License.
Abstract
Background: White spot lesions (WSLs) are a problem commonly found in patients who use orthodontic devices. Fluoride varnish can reduce WSLs during orthodontic treatment with fixed appliances. The aim of this systematic review was to evaluate the efficacy of fluoride varnish compared with other agents for preventing WSLs during orthodontic treatment.
Methods: Studies were searched from four databases- PubMed, Scopus, Web of Science and Cochrane Library- from January 1980 to May 2017; only studies with English abstracts were included.
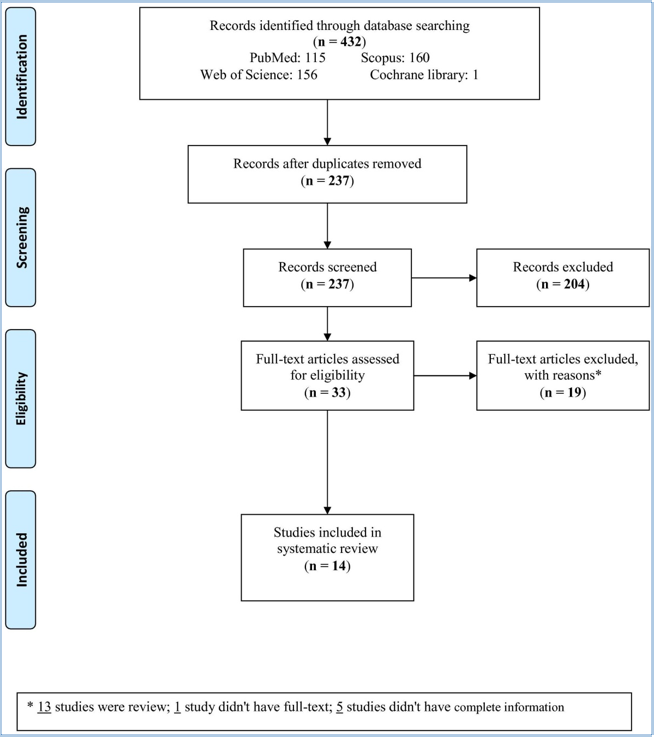
Results: Out of 432 studies searched from the databases, 33 studies were evaluated for eligibility. Of the 33 studies, 19 were excluded with reasons and 14 studies were included in the systematic review. Parameters of WSLs (decalcification score, prevalence, incidence, progression score, ΔQ and ΔZ and DiagnoDent (DD) pen score) were compared for the various treatments.
Conclusions: Although there were some limitations for this systematic review study, the review showed that fluoride varnish combined with chlorhexidine (CHX) may be a good treatment for WSLs after orthodontic treatment, especially for a 6-month period, and that resin infiltration might also be effective for preventing WSLs. More studies are needed to further investigate these observations.
Introduction
Fixed orthodontic appliances create stagnation areas for plaque and thus difficulties for tooth cleaning. Moreover, the irregular and non-uniform surfaces of brackets, bands and wires limit the naturally occurring self-cleansing mechanism of the oral musculature and saliva Mount et al., 2016. White spot lesions (WSLs) are a problem commonly found in patients who use orthodontic devices. While it takes around 6 months for caries to progress in a patient not submitted to orthodontic therapy, it takes around 1 month for those who are Lucchese and Gherlone, 2012. WSLs progress around orthodontic ligatures, brackets and bands because these appliances physically prevent thorough dental cleaning and potentiate bacterial biofilm accumulation on tooth surfaces Lucchese and Gherlone, 2012Tufekci et al., 2011. Suitable preventative agents or treatments for WSLs or caries have typically fluoride products (e.g. toothpaste, varnishes, gels and mouth rinse), antimicrobials (e.g. chlorhexidine (CHX)), diet counseling, xylitol gum and casein derivatives Derks et al., 2004. Topical fluoride varnishes can reduce WSLs during orthodontic treatment and they are assumed to have the same effect following orthodontic therapy Stecksén-Blicks et al., 2007. The aim of this systematic review herein was to evaluate the efficacy of fluoride varnish, compared to other treatments, for preventing WSLs during orthodontic treatment with fixed appliances.
Materials - Methods
Search strategies and study criteria
The studies were searched from four databases (PubMed, Scopus, Web of Science and Cochrane Library) from January 1980 to May 2017. Only publications with English abstracts were included. The search keywords were "orthodontic treatment" and "white spot" and "fluoride".
Study selection
One author (M.S.) conducted the initial search for articles, with a second author (H.R.M.) blinded to the first author’s search. If there was any disagreement between the two authors, the third author (F.R.) resolved the problem. All articles included in the study review were subjected to evaluation for any indication of the efficacy of fluoride varnish after orthodontic treatment. Only studies with abstracts written in English were included in the review.
Data extraction
The name of the author, year of publication, country, parameters of WSLs, the comparison of groups, and P-values were the relevant data extracted from each study. A P-value<0.05 was considered to be statistically significant.
Results
Study characteristics
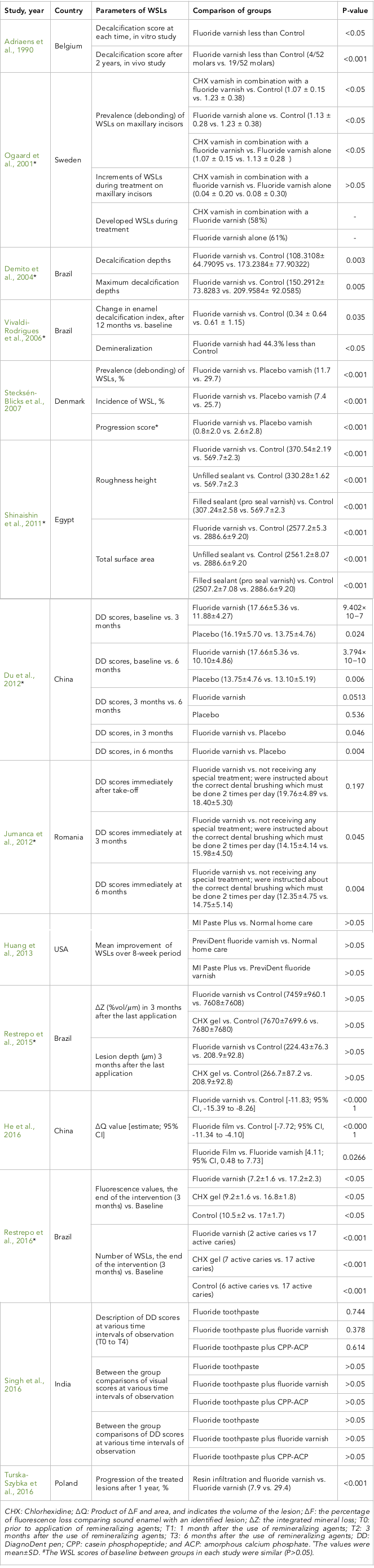
The flowchart of the study selection is shown in Figure 1 . Of the 432 studies searched among the databases, 33 studies were evaluated for eligibility. Of the 33 studies, 19 were excluded for several reasons (e.g. articles were reviews and not original studies, they did not have available full-text, or they contained incomplete information) ( Figure 1 ). Thus, the remaining 14 studies were included in the systematic review ( Table 1 ). The studies were reported from 1990 to 2016. Of these reported studies, 1 was from Belgium, 1 from Sweden, 4 from Brazil, 1 from Denmark, 1 from Egypt, 2 from China, 1 from Romania, 1 from the USA, 1 from India, and 1 from Poland.
Parameters of WSLs
Decalcification Score
This score was significantly less for fluoride varnish than for control in an in vitro study and after 2 years of an in vivo study Adriaens et al., 1990. Another study reported that decalcification depths and maximum decalcification depths were significantly lower in fluoride varnish compared to control Øgaard et al., 2001. The change in the enamel decalcification index after 12 months vs. baseline was less for fluoride varnish vs. control (P=0.035) Vivaldi-Rodrigues et al., 2006.
Prevalence and Incidence
Prevalence (debonding) of WSLs on maxillary incisors was significantly less for CHX varnish combined with fluoride varnish, for fluoride varnish compared to control, and also for CHX varnish combined with fluoride varnish compared to fluoride varnish alone Demito et al., 2004. This prevalence was 11.7% for fluoride varnish versus 29.7% for placebo varnish (P<001) Stecksén-Blicks et al., 2007. The incidence of WSLs was 7.4% for fluoride varnish vs. 25.7% for placebo varnish (P<0.001) Stecksén-Blicks et al., 2007. The number of WSLs at the end of the intervention (3 months) versus baseline was less for fluoride varnish compared to control, or for control compared to CHX gel Restrepo et al., 2016.
Progression score
Increments of WSLs during treatment on maxillary incisors for CHX varnish combined with fluoride varnish was less than the increments for fluoride varnish alone (P<0.05); progression of WSLs was 58% vs. 61% Øgaard et al., 2001, whereas was it was 0.8% for fluoride varnish vs. 2.6% for placebo varnish (P<0.001) Stecksén-Blicks et al., 2007. The mean improvement of WSLs over the 8-week period for MI Paste Plus and fluoride varnish were less than that for normal home care; the mean improvement of WSLs for MI Paste Plus was less than for fluoride varnish (P<0.05) Huang et al., 2013. Progression of the treated lesions after one year was 7.9% in resin infiltration combined with fluoride varnish compared to 29.4% for fluoride varnish alone (P<0.001) Turska-Szybka et al., 2016.
Q and Z
Q value was significantly less for fluoride varnish and fluoride film compared to control, and also less for fluoride varnish compared to fluoride film He et al., 2016. Indeed, Z in 3 months after the last application of fluoride varnish and CHX gel was less than for control (P>0.05), Z for fluoride varnish was less than that of CHX gel (P>0.05). However, lesion depth in 3 months after the last application of control was less than that for fluoride varnish and CHX gel (P>0.05); lesion depth for CHX was less than that for fluoride varnish (P>0.05) Restrepo et al., 2015. Demineralization in fluoride varnish was 44.3% less than that for control Vivaldi-Rodrigues et al., 2006 . Fluorescence value at the end of the intervention (3 months) vs. baseline was (7.2±1.6 vs. 17.2±2.3), (9.2±1.6 vs. 16.8±1.8), and (10.5±2 vs. 17±1.7) for fluoride varnish, CHX gel, and control, respectively (P<0.05). These values were less than fluoride varnish compared to CHX gel after 3 months, and compared to baseline Restrepo et al., 2016.
DD Scores
DD scores in 3 months and 6 months (versus baseline) were less for fluoride varnish and placebo, and also less for 6 months compared to 3 months (P<0.05) Restrepo et al., 2015. At these two time points, the DD score of fluoride varnish was less than that of placebo (P<0.05) Restrepo et al., 2015. Additionally, DD scores for 3 months and 6 months (versus baseline) were less for fluoride varnish compared to placebo (P<0.05), and less for 6 months compared to 3 months Jumanca et al., 2012. DD and visual scores at various time intervals of observation (prior to application, 1 month, 3 months and 6 months) for fluoride toothpaste, fluoride toothpaste + fluoride varnish, fluoride toothpaste + DiagnoDent pen, casein phosphopeptide (CPP), and amorphous calcium phosphate (CPP-ACP) were not different (P>0.05). Moreover, DD scores between treatment groups at various time intervals of observation were not different (P>0.05) Singh et al., 2016.
Other
Roughness height and total surface area of WSLs after fluoride varnish, unfilled sealants and filled sealants (pro-seal varnish) were all less than control (P<0.001). Also, roughness height for filled sealant (pro-seal varnish) was less than that for unfilled sealant, while roughness height for unfilled sealant was less than that for fluoride varnish. The total surface area for unfilled sealant was less than that for fluoride varnish; and total surface area for fluoride varnish was less than filled sealant (pro-seal varnish) Shinaishin et al., 2011.
Discussion
This systematic review evaluated the efficacy of fluoride varnish for preventing WSLs during orthodontic treatment and compared its efficacy to other treatments. The results indicated that fluoride varnish was an effective treatment for orthodontic patients, compared to patients without treatment (control or placebo). By increasing treatment time (of fluoride varnish) to 6 months, one can reduce WSLs; thus, 6 months of fluoride varnish was more effective than a shorter treatment time. Importantly, fluoride varnish combined with CHX was more effective than fluoride varnish alone.
The prevalence of WSLs in patients that seek orthodontic treatment is in the range of 50% to 96% Geiger et al., 1992Øgaard et al., 1996Vivaldi-Rodrigues et al., 2006. Lucchese and Gherlone (2013) showed that the first 6 months are of particular importance in the development of WSLs because the majority of adolescent patients need to adapt their hygienic practices to the requirements of orthodontic therapy. It is assumed that calcium, fluoride and phosphate will penetrate the deepest areas of lesions Llena-Puy, 2013.
Fluoride varnishes have been suggested to be safe and feasible for topical application. They include high concentrations of fluoride (not the fluoride used daily in toothpaste and mouth rinse). The varnish may also remain on tooth surfaces for several hours after application, and may be capable of releasing sufficiently high concentrations of fluoride ions to maintain surface fluoridation Seppä, 1983. One study Farhadian et al., 2008 revealed a 40% reduction in depth of demineralization around brackets after application of high concentration fluoride varnish. Many clinicians have applied topical fluoride to WLSs as the first step in treatment.
When the pH of oral fluids increases to normal levels, the calcium and phosphate ions of saliva are transmitted through the pellicle into the enamel; according to the laws of chemical equilibrium, this leads to remineralization de Leeuw, 2004. Certainly, this process is greatly enhanced by fluoride in saliva and plaque. Another study McNeill et al., 2001 reported that fluoride inhibits mineral loss during the acid dissolution process and enhances remineralization in a similar manner to that which occurs in dental enamel.
The benefits of using antimicrobial agents for the control of gingivitis have been widely discussed in the literature, and at present, CHX is considered the most effective agent for this purpose Sari and Birinci, 2007. CHX has the capacity to prevent biofilm formation, which is one of the main etiological factors of caries disease. However, CHX affects the prevention and control of WSLs Twetman, 2004. In a short-term in vivo study, a combination of daily mouth rinsing with fluoride and CHX was more effective at decreasing mineral loss and lesion development than fluoride mouth rinsing alone Ullsfoss et al., 1994. Huizinga et al. (1991) calculated that CHX would be need to be released from the varnish for at least 6 months after a topical application Huizinga et al., 1991. Some studies have shown the efficacy of CHX varnishes in decreasing the prevalence of caries during orthodontic treatment, yet other studies have not shown the efficacy of a varnish of 40% CHX Kronenberg et al., 2009Øgaard et al., 2001. Moreover, the main benefits of CPP-ACP are their ability to localize at the tooth’s surface and penetrate into the supragingival plaque to provide bioavailable calcium and phosphate ions where they are most needed Reynolds et al., 2003.
Turska-Szybka et al. (2016) concluded that resin infiltration in conjunction with fluoride varnish treatment of early facial smooth-surface caries lesions in deciduous teeth is superior to fluoride varnish treatment alone for reducing lesion progression Turska-Szybka et al., 2016. The studies Hammad et al., 2012Mueller et al., 2006Paris and Meyer-Lueckel, 2010 showed a good effect of resin infiltration on WSLs after debonding orthodontic brackets. The studies concluded that treatment with resin infiltration in conjunction with fluoride varnish is promising for controlling proximal lesions Ekstrand et al., 2010 and in fact, teeth treated with resin infiltration showed higher Vickers hardness values than untreated teeth Palamara, 2010. Based on our knowledge, there were no study on the efficacy of resin infiltration versus fluoride varnish+ CHX for WSL treatment; therefore, more studies in the future are necessary to follow up on this comparison.
Limitations of this systematic review included: (1) heterogeneity between the studies; (2) difference in age and sex between the studies; (3) few studies reported the efficacy of a type of treatment compared with other treatments; (4) many parameters of WSLs in the studies; and (5) different types of study environment (in vitro and in vivo). The studies concluded that treatment with resin infiltration in conjunction with fluoride varnish is promising for controlling proximal lesions
Conclusion
While this systematic review has several limitations, it also demonstrates that fluoride varnish combined with CHX could be an effective treatment for WSLs after orthodontic procedure. It is best that fluoride varnish be available for 6-month period of treatment, at least. The study review also demonstrated or concluded that treatment with resin infiltration in conjunction with fluoride varnish is a promising combination for controlling proximal lesions (e.g. WSLs). More studies in the future are needed to explore that.
Abbreviations
WSL: White spot lesion
CHX: Chlorhexidine
Q: Product of F and area
F: The percentage of fluorescence loss comparing sound enamel with an identified lesion
Z: The integrated mineral loss
T: Time
DD: DiagnoDent
CPP: Casein phosphopeptide
ACP: Amorphous calcium phosphate
SD: Standard deviation
Author Contribution
All authors drafted the first version and approve the final draft.
References
-
M.
Adriaens,
L.
Dermaut,
R.
Verbeeck.
The use of ‘Fluor Protector®’, a fluoride varnish, as a caries prevention method under orthodontic molar bands. The European Journal of Orthodontics.
1990;
12
:
316-319
.
-
N.H.
Leeuw.
Resisting the onset of hydroxyapatite dissolution through the incorporation of fluoride. The Journal of Physical Chemistry B.
2004;
108
:
1809-1811
.
-
C.
Demito,
G.
Vivaldi-Rodrigues,
A.
Ramos,
S.
Bowman.
The efficacy of a fluoride varnish in reducing enamel demineralization adjacent to orthodontic brackets: an in vitro study. Orthodontics & craniofacial research.
2004;
7
:
205-210
.
-
A.
Derks,
C.
Katsaros,
J.
Frencken,
M.
Van’t Hof,
A.
Kuijpers-Jagtman.
Caries-inhibiting effect of preventive measures during orthodontic treatment with fixed appliances. Caries research.
2004;
38
:
413-420
.
-
K.
Ekstrand,
A.
Bakhshandeh,
S.
Martignon.
Treatment of proximal superficial caries lesions on primary molar teeth with resin infiltration and fluoride varnish versus fluoride varnish only: efficacy after 1 year. Caries research.
2010;
44
:
41-46
.
-
N.
Farhadian,
A.
Miresmaeili,
B.
Eslami,
S.
Mehrabi.
Effect of fluoride varnish on enamel demineralization around brackets: an in-vivo study. American Journal of Orthodontics and Dentofacial Orthopedics.
2008;
133
:
S95-S98
.
-
A.M.
Geiger,
L.
Gorelick,
A.J.
Gwinnett,
B.J.
Benson.
Reducing white spot lesions in orthodontic populations with fluoride rinsing. American Journal of Orthodontics and Dentofacial Orthopedics.
1992;
101
:
403-407
.
-
S.M.
Hammad,
M.
El Banna,
I.
El Zayat,
M.A.
Mohsen.
Effect of resin infiltration on white spot lesions after debonding orthodontic brackets. Am J Dent.
2012;
25
:
3-8
.
-
T.
He,
X.
Li,
Y.
Dong,
N.
Zhang,
Y.
Zhong,
W.
Yin,
D.
Hu.
Comparative assessment of fluoride varnish and fluoride film for remineralization of postorthodontic white spot lesions in adolescents and adults over a 6-month period: A single-center, randomized controlled clinical trial. American Journal of Orthodontics and Dentofacial Orthopedics.
2016;
149
:
810-819
.
-
G.J.
Huang,
B.
Roloff-Chiang,
B.E.
Mills,
S.
Shalchi,
C.
Spiekerman,
A.M.
Korpak,
J.L.
Starrett,
G.M.
Greenlee,
R.J.
Drangsholt,
J.C.
Matunas.
Effectiveness of MI Paste Plus and PreviDent fluoride varnish for treatment of white spot lesions: a randomized controlled trial. American Journal of Orthodontics and Dentofacial Orthopedics.
2013;
143
:
31-41
.
-
E.
Huizinga,
J.
Ruben,
J.
Arends.
Chlorhexidine and thymol release from a varnish system. Journal de biologie buccale.
1991;
19
:
343-348
.
-
D.
Jumanca,
A.
Galuscan,
A.C.
Podariu,
L.
Ardelean,
L.C.
Rusu.
Infiltration Therapy-an Alternative to Fluoride Varnish Application for Treatment of White Spot Lesion After Fixed Orthodontic Treatment. Revista de Chimie.
2012;
63
:
783-786
.
-
O.
Kronenberg,
A.
Lussi,
S.
Ruf.
Preventive effect of ozone on the development of white spot lesions during multibracket appliance therapy. The Angle orthodontist.
2009;
79
:
64-69
.
-
C.
Llena-Puy.
MI Paste Plus and PreviDent fluoride varnish appear No more effective than normal home care for improving the appearance of white spot lesions. Journal of Evidence Based Dental Practice.
2013;
13
:
114-116
.
-
A.
Lucchese,
E.
Gherlone.
Prevalence of white-spot lesions before and during orthodontic treatment with fixed appliances. European Journal of Orthodontics.
2012;
35
:
664-668
.
-
C.J.
McNeill,
W.A.
Wiltshire,
C.
Dawes,
C.L.
Lavelle.
Fluoride release from new light-cured orthodontic bonding agents. American Journal of Orthodontics and Dentofacial Orthopedics.
2001;
120
:
392-397
.
-
G.J.
Mount,
W.R.
Hume,
H.C.
Ngo,
M.S.
Wolff.
Preservation and restoration of tooth structure. John Wiley & Sons.
2016
.
-
J.
Mueller,
H.
Meyer-Lueckel,
S.
Paris,
W.
Hopfenmuller,
A.
Kielbassa.
Inhibition of lesion progression by the penetration of resins in vitro: influence of the application procedure. Operative dentistry.
2006;
31
:
338-345
.
-
B.
Øgaard,
H.
Duschner,
J.
Ruben,
J.
Arends.
Microradiography and confocal laser scanning microscopy applied to enamel lesions formed in vivo with and without fluoride varnish treatment. European journal of oral sciences.
1996;
104
:
378-383
.
-
B.
Øgaard,
E.
Larsson,
T.
Henriksson,
D.
Birkhed,
S.E.
Bishara.
Effects of combined application of antimicrobial and fluoride varnishes in orthodontic patients. American Journal of Orthodontics and Dentofacial Orthopedics.
2001;
120
:
28-35
.
-
J.E.
Palamara,
M.
Tyas,
M.F.
Burrow.
Resin infiltrated artificial caries lesions examined by polarized light microscopy and micro-hardness tests. Hamburg, Germany: DMG.
2010
.
-
S.
Paris,
H.
Meyer-Lueckel.
Inhibition of caries progression by resin infiltration in situ. Caries research.
2010;
44
:
47-54
.
-
M.
Restrepo,
D.
Bussaneli,
F.
Jeremias,
R.
Cordeiro,
D.
Raveli,
A.
Magalhães,
C.
Candolo,
L.
Santos-Pinto.
Control of white spot lesions with use of fluoride varnish or chlorhexidine gel during orthodontic treatment a randomized clinical trial. Journal of Clinical Pediatric Dentistry.
2016;
40
:
274-280
.
-
M.
Restrepo,
D.G.
Bussaneli,
F.
Jeremias,
R.C.
Cordeiro,
A.C.
Magalhães,
D.M.
Palomari Spolidorio,
L.
Santos-Pinto.
Control of white spot lesion adjacent to orthodontic bracket with use of fluoride varnish or chlorhexidine gel. The Scientific World Journal.
2015;
2015
.
-
E.
Reynolds,
F.
Cai,
P.
Shen,
G.
Walker.
Retention in plaque and remineralization of enamel lesions by various forms of calcium in a mouthrinse or sugar-free chewing gum. Journal of dental research.
2003;
82
:
206-211
.
-
E.
Sari,
I.
Birinci.
Microbiological evaluation of 0.2% chlorhexidine gluconate mouth rinse in orthodontic patients. The Angle Orthodontist.
2007;
77
:
881-884
.
-
L.
Seppä.
Effect of dental plaque on fluoride uptake by enamel from a sodium fluoride varnish in vivo. Caries research.
1983;
17
:
71-75
.
-
S.F.
Shinaishin,
S.A.
Ghobashy,
T.H.
EL-Bialy.
Efficacy of light-activated sealant on enamel demineralization in orthodontic patients: an atomic force microscope evaluation. The open dentistry journal.
2011;
5
:
179
.
-
S.
Singh,
S.P.
Singh,
A.
Goyal,
A.K.
Utreja,
A.K.
Jena.
Effects of various remineralizing agents on the outcome of post-orthodontic white spot lesions (WSLs): a clinical trial. Progress in orthodontics.
2016;
17
:
25
.
-
C.
Stecksén-Blicks,
G.
Renfors,
N.
Oscarson,
F.
Bergstrand,
S.
Twetman.
Caries-preventive effectiveness of a fluoride varnish: a randomized controlled trial in adolescents with fixed orthodontic appliances. Caries research.
2007;
41
:
455-459
.
-
E.
Tufekci,
J.S.
Dixon,
J.
Gunsolley,
S.J.
Lindauer.
Prevalence of white spot lesions during orthodontic treatment with fixed appliances. The Angle orthodontist.
2011;
81
:
206-210
.
-
A.
Turska-Szybka,
D.
Gozdowski,
E.
Mierzwińska-Nastalska,
D.
Olczak-Kowalczyk.
Randomised Clinical Trial on Resin Infiltration and Fluoride Varnish vs Fluoride Varnish Treatment Only of Smooth-surface Early Caries Lesions in Deciduous Teeth. Oral health & preventive dentistry.
2016;
14
:
485-491
.
-
S.
Twetman.
Antimicrobials in future caries control? A review with special reference to chlorhexidine treatment. Caries Res.
2004;
38
:
223-229
.
-
B.N.
Ullsfoss,
B.
Ögaard,
J.
Arends,
J.
Ruben,
G.
Rölla,
J.
Afseth.
Effect of a combined chlorhexidine and NaF mouthrinse: an in vivo human caries model study. European Journal of Oral Sciences.
1994;
102
:
109-112
.
-
G.
Vivaldi-Rodrigues,
C.F.
Demito,
S.J.
Bowman,
A.L.
Ramos.
The effectiveness of a fluoride varnish in preventing the development of white spot lesions. World journal of orthodontics.
2006;
7
.
Comments

Downloads
Article Details
Volume & Issue : Vol 4 No 08 (2017)
Page No.: 1513-1526
Published on: 2017-08-25
Citations
Copyrights & License
This work is licensed under a Creative Commons Attribution 4.0 International License.
Search Panel
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Search for this article in:
Google Scholar
Researchgate
- HTML viewed - 11535 times
- Download PDF downloaded - 3155 times
- View Article downloaded - 14 times

{kind=link}
{kind=link}