

Copyrights: Seyed Ahmad Hosseinzadeh, Shahrzad Mazhari, Kiomars Najafi, Meysam Ahmadi, Iraj Aghaei, Mojtaba Khaksarian, 2018. License: This work is licensed under a Creative Commons Attribution 4.0 International License.
Abstract
Introduction: Stroke is one of the most serious and debilitating diseases in our society. Stroke survivors can suffer several neurological impairments. They typically show pathological changes in neural functions of brain areas. Transcranial direct current stimulation (tDCS) can be applied to modify cerebral excitability and has been recently applied in the treatment of neuropsychological and neurological disorders. The aim of the study herein was to evaluate changes in movement and cognitive functions of chronic ischemic stroke patients using anodic and cathodic tDCS.
Method: In this clinical trial, 100 patients with chronic ischemic stroke were divided in 4 groups (control, sham, anodic tDCS, and cathodic tDCS; n=25 per group). The patients underwent routine treatment and received the same tDCS protocol (3 times per week of 30-min sessions during one month). Movement and cognitive functions were evaluated using the NIHSS Scale & Trail Making Test and the Beck Test, before and after 1 and 3 months of tDCS sessions. All data were analyzed by 2-way repeated measures ANOVA using SPSS program (version 18).
Results: The results showed that there were significant increases (P<0.001) in NIHSS score and Barthel index between anodic group versus control, sham, or cathodic group, at various timepoints (before vs. 1 month after tDCS, 1 month vs. 3 months after tDCS, and before vs. 3 months after tDCS). Furthermore, there were significant decreases (P<0.001) between anodic group versus control, sham, or cathodic group, at the various timepoints (before vs. 1 month after tDCS, 1 month vs. 3 months after tDCS, and before vs. 3 months after tDCS).
Conclusion: Anodic tDCS has advantageous effects on movement and cognitive rehabilitation in stroke patients, but future studies are needed to further discern the differences and develop precise treatment protocols.
Introduction
Stroke is one of the most serious and debilitating diseases of our time, and causes motor and cognitive impairment in patients. Approximately 50% to 60% of patients with stroke will experience some degree of motor impairment 12. Stroke can induce its unpleasant effects on different areas of the brain; the affected areas can be discerned depending on the various clinical manifestations. The treatment strategies for stroke are mainly focused on prevention of further injuries and on rehabilitation for the patients.
In the early stages of acute stroke, about two-thirds of patients show signs of motor disabilities. A few weeks after the stroke, a new organization is created in the brain. However, many of the motor and cognitive problems still remain and do not respond adequately to existing drug and rehabilitation medications. Studies using functional magnetic resonance imaging (FMRI) in people with stroke have shown that abnormal patterns in the cortex, such as in the language domains, are observed in these patients 3. Patients also show evidence of increase in pathologic trends of both healthy and affected hemispheres 3. The membrane polarization change can, in turn, lead to diverse changes in single-neuron synaptic and network activity, which may ultimately reflect behavioral and cognitive changes 4. In recent years, transcranial direct current stimulation (tDCS) has been applied in treatment of neuropsychological and neurological disorders.
Furthermore, depression can occur in patients with stroke and represents another problem in this group of patients. The depression usually lasts for weeks to months after the disease, and is reported to occur in about 11% of patients 5. In some studies, the remaining symptoms of depression, including mood disorders, negative attitudes to life have been reported in about 40% of patients 6. Also, the results of studies on post-stroke depression have indicated an increase in mortality rates in people of 65 years of age and older 5. Clinically-defined vascular depression was proposed 56, and such diagnosis was validated on the basis of the presence of sub-cortical pathology and white matter hyper intensities in MRI scans. Patients with a higher age who have vascular problems also exhibit more cognitive impairment than geriatric patients without non-vascular depression.
The main goal of tDCS is to increase stimulation of the nerve cells in the affected hemisphere. A tDCS flows toward M1 lesioned hemisphere. Behavioral gains were accompanied by enhanced cortical excitability and reduced intracranial inhibition within M1 lesioned hemisphere, suggesting the involvement of glutamatergic and GABAergic neurotransmission as possible operating mechanisms in the cathode, due to the excess of positive ions, such as sodium ions, and their combination with water 564.
However, while tDCS has been applied for neuropsychological and neurological disorder treatment in recent years, the results of tDCS application for stroke patients and its effects have been controversial in the literature. Some studies have shown positive effects of anodic tDCS on corticospinal excitability 4, upper limb motor recovery 7, and movement learning after stroke 8. Moreover, there have been improvement of precision grip and dexterity of the paretic hand 9, increase of knee extensor force 10, enhanced facilitation of motor recovery 11, improved performance of motor sequence tasks after chronic stroke 12, and improvement in motor skill learning 13. On the other hand, some studies have shown the positive effects of cathodic tDCS. For example, a neuroprotective effect of cathodal tDCS in a rat stroke model has been shown 3 14, as well as improvement of hand dexterity and selective attention 15, and post-stroke unilateral visuospatial neglect 3.
Moreover, controversial findings in research have been reported about tDCS effects on post-stroke depression. For example, in two studies conducted by researchers, the positive effects of anodic tDCS in 522 and 141 patients with chronic stroke were studied; it was observed that the use of this method was able to create positive changes in attitude towards life and hope for life31516. On the other hand, some studies of this group of patients who used anodic tDCS to reduce the negative effects of depression showed that this method was not able to produce specific and positive effects in reducing the complications of post-stroke depression 17.
Therefore, the current research study was designed using well-known motor and cognitive criteria to provide a better understanding of the anodic and cathodic tDCS functions with respect to improving motor, cognitive functions, and depression in chronic stroke patients.
Methods
Subjects
This study is an interventional and clinical trial study that was prospective, double-blinded, and controlled (included sham). In order to observe the double-blindness of the research, the patients chose closed envelopes for the rhombus, in which specific codes were inserted. The patients and tDCS-conducting technicians did not know the content of the envelopes, thus providing a satisfactory classification of the four groups. The research groups (of patients) were based on the random selection of envelopes.
The 100 patients (male & female; of age between 41-75 years) were divided in 4 groups. All subjects were patients with chronic ischemic stroke who were admitted at the Tolou Clinic, Rasht, Iran. Magnetic resonance imaging (MRI) was performed to confirm both lesion locations. Patients with other types of stroke were not included to reduce the heterogeneity of the study population.
We assessed the changes in movement and cognitive functions of the stroke patients using NIHSS scales (National Institute of Health Stroke Scale) for movement function evaluation, Trail Making Test (a visual attention assessment test), and Beck Test (for depression evaluation). Patients with a heart pacemaker or metal implants, seizure, drug-resistance epilepsy, brain tumors, dementia, drug abuse, and severe cognitive deficits were excluded from the study, as were those using neuroactive or psychoactive drugs, implant pumps, stimulators or shunts. All patients took routine drugs and medications (such as physiotherapy), and were divided randomly into 4 groups: 1) control (routine treatment only), 2) sham, 3) anodic tDCS, and 4) cathodic tDCS.
Transcranial Direct Current Stimulation (tDCS)
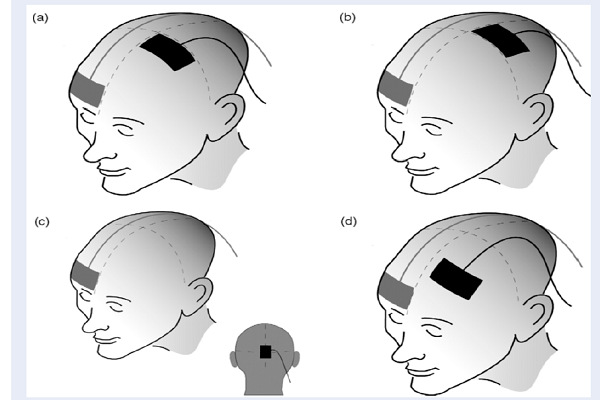
tDCS was applied by a battery-powered, constant current electrical stimulator (at 2-mA intensity using a pair of surface saline-soaked 35-cm2 sponge electrodes (5 × 7 cm), for 3 times a week for 1 month, for 30 min per session and at an electric current of 2 mA. We used two different electrode montages, including an anode and a cathode. In anodal tDCS, the anode electrode was mounted on the left superior temporal gyrus, while the cathode was placed over the contralateral superior region (cp5). The current was run through the brain and other tissues of the head, from the anode to the cathodal electrode. In cathodal tDCS, the cathode was used for placement symmetrical to the left gyrus (cp6), while the anode was placed at the contralateral supraorbital region. In sham tDCS, the anode was placed over the left superior temporal gyrus and cathode was placed on the contralateral supraorbital region, but no current was applied (Figure 1). All patients received the same protocol, 3 times a week for 30 min per session for 1 month. Then, all of these evaluation tests were applied for the patients at 3 months after ending the tDCS sessions.
Experimental procedure
All participants performed a movement function scale (NIHSS) and a visual attention test (Trail Making Test) and Beck Test (for depression evaluation), before, after and 3 months after tDCS sessions.
NIHSS scale
NIHSS is a stroke scale with eleven levels for measuring the severity of motor disorders that are widely used in clinical trials.
Trail Making Test
The Trail Making Test is a measure to examine the speed of cognitive processing and visual attention.
Beck Test
The Beck depression scale is one of the most widely used standards for assessing the severity of depression in patients. It is based on a questionnaire with 21 multiple choice questions in which the severity of depression is proportional to the patient score.
Statistical Analysis
All data were expressed as mean ± SEM and analyzed using SPSS software, version 18 (IBM, USA). Two-way repeated measures ANOVA was applied for assessment of differences between groups, time of treatment, and interaction group × time of treatment. Individual comparisons were performed by Tukey's test. A value of P<0.05 was considered to be statistically significant.
Results
We evaluated 100 ischemic stroke patients that were diagnosed with movement and cognitive impairments. These patients had many changes in movement and cognitive functions. The post-stroke onset in these patients was between 25-180 days. All patients were randomized into 4 groups: control (n=25), sham (n=25), anodic tDCS (n=25), and cathodic tDCS (n=25).
| Group | ||||||||
| Control | Sham | Anodic | Cathodic | Total | P | |||
| Sex 1 | Female | Count | 13 | 13 | 12 | 13 | 51 | 0.989 |
| Column N % | 52.0% | 52.0% | 48.0% | 52.0% | 51.0% | |||
| Male | Count | 12 | 12 | 13 | 12 | 49 | ||
| Column N % | 48.0% | 48.0% | 52.0% | 48.0% | 49.0% | |||
| Total | Count | 25 | 25 | 25 | 25 | 100 | ||
| Column N % | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | |||
| Lesion Side 1 | Left | Count | 15 | 14 | 14 | 14 | 57 | |
| Column N % | 60.0% | 56.0% | 56.0% | 56.0% | 57.0% | |||
| Right | Count | 10 | 11 | 11 | 11 | 43 | ||
| Column N % | 40.0% | 44.0% | 44.0% | 44.0% | 43.0% | 0.989 | ||
| Total | Count | 25 | 25 | 25 | 25 | 100 | ||
| Column N % | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% | |||
| Age | Mean | 59 | 59 | 58 | 60 | 59 | 0.718 | |
| Standard Deviation | 8 | 7 | 8 | 7 | 7 | |||
| Minimum | 42 | 42 | 46 | 45 | 42 | |||
| Maximum | 75 | 71 | 71 | 72 | 75 |
There were no differences in gender, age, or time of post-stroke onset among all the groups. Table 1 summarizes the numeric value means of these groups (control, sham, anodic and cathodic). All selected patients were of ages between 40-75 years, and had been diagnosed with stroke in the subcortical and ischemic middle cerebral artery territory. Participants tolerated the applied currents under the different conditions very well and there was no interruption of experimental procedures due to adverse or side effects of the applied currents.
The two-way repeated measures ANOVA showed that there were significant differences among the control, sham, anodic tDCS, and cathodic tDCS groups before initiation of the tDCS treatment protocol; the time of treatment was significant for all groups (P<0.001). Furthermore, the interaction group × time treatment was significant for three tests, thus indicating the effects of the groups on treatment are different and dependent on time period. The analysis are mentioned in the section of each test.

Anodic and cathodic tDCS effects on NIHSS test
The results of the two-way repeated measures ANOVA showed that there are very significant differences between groups before initiation of tDCS protocol and within groups or treatment time (P<0.0001). Furthermore, the interaction group x treatment time was significant (P<0.0001), indicating that the effects of groups at different times were significant on rehabilitation of chronic stroke. Therefore, we applied 2-way repeated measures ANOVA test for assessment of difference at various time-points: from before to 1 month after tDCS, from 1 month to 3 months after tDCS, and from before to 3 months after tDCS, and evaluated these for all the groups to discern differences. The results of the two-way repeated measures ANOVA followed by Tukey’s HSD test showed significant differences in NIHSS scores at three time-points: from before 1 month after tDCS, from 1 month to 3 months after tDCS, and from before to 3 months after tDCS. There was a significant increase observed between anodic tDCS group versus control, sham and cathodic tDCS groups (P<0.001. However, when comparing the cathodic tDCS group with sham, the difference of NIHSS score was significantly decreased by two times, at the time-points from before to 1 month after tDCS and from before to 3 months after tDCS (P<0.05 and 0.001, respectively) (Figure 2).

Anodic and cathodic tDCS effects on Trail Making Test
The results of the two-way repeated measures ANOVA showed that there are very significant differences between groups before initiation of the tDCS protocol and within groups or treatment times (P<0.0001). Furthermore, the interaction group × treatment time was significant (P<0.0001) that these indicated the effects of groups at different times were significant on the rehabilitation of chronic stroke. Therefore, we applied repeated measures ANOVA test for assessment of the different time-points (from before to 1 month after tDCS, from 1 month to 3 months after tDCS, and from before to 3 months after tDCS protocol); these were evaluated and compared among all the groups. The results of the two-way repeated measures ANOVA followed by Tukey’s HSD test showed that a significant difference by the Trail Making Test at three time-points: before — 1 month after tDCS, 1 month — 3 months after tDCS, and before — 3 months after tDCS. There was a significant increase between the anodic tDCS group versus control, sham, or cathodic tDCS groups (P<0.001). Furthermore, the difference of the Trail Making Test in cathodic tDCS group, compared with the sham group, was significantly decreased, from before to 1 month after tDCS treatment, and from before to 3 months after tDCS treatment (P<0.01 and 0.05 respectively) (Figure 3).

Anodic and cathodic tDCS effects on Beck test
The results of the two-way repeated measures ANOVA showed there are very significant differences between the groups before the initiation of the tDCS protocol and within the groups or treatment times (P<0.0001). Furthermore, the interaction group × treatment time was significant (P<0.0001), indicating that the effects of the groups at different times were significant on rehabilitation of chronic stroke. The effects of anodic and cathodic tDCS on the difference/change of the Beck test of the groups were evaluated for three time-points: from before to 1 month after tDCS, from 1 month to 3 months after tDCS, and from before to 3 months after tDCS treatment. We applied 2-way repeated measures ANOVA test for assessment of differences between the groups for these time-points. The results of the ANOVA test followed by Tukey’s HSD test showed a significant difference of the Beck test, at the time period before tDCS to 1 month after DCS. There was a significant decrease observed in the Beck test between the anodic tDCS group versus control, sham, and cathodic tDCS groups (P<0.001). Furthermore, the difference of the Beck test in the cathodic tDCS group, versus sham group, was significantly decreased at the time period from before to 1 month after tDCS, from 1 month to 3 months after tDCS, and 0 – 3 months after tDCS (P<0.0001) (Figure 4).

Discussion
The results of the study herein show that anodic tDCS application could lead to positive improvements of movement (based on NIHSS scores), visual attention (based on the Trail Making Test), and depression (based on the Beck Test). Although we do not know the exact cause or mechanisms of the effects of tDCS on movement, visual attention and depression, our findings show that this procedure has multiple positive facets on rehabilitation of chronic stroke patients. Our research — and also of other similar studies- shows that anodic tDCS have beneficial effects on stroke. The importance of the results obtained in this study is the relevance to the target groups (65 and older), who have in recent years, shown an ever-increasing rise in the number of debilitating illnesses, which lead to great economic, social and human costs on society, and which have become a widespread problem for field activists. Therefore, any success in treating diseases such as stroke, using modern, low-cost and least invasive methods like tDCS, can provide promising horizons for treating or reducing impotence after a stroke. These therapies will help advance the understanding of chronic ischemic stroke by researchers, therapists, and patients.
Research has already shown that anodic tDCS can benefit patients with chronic stroke 7. A study in stroke survivors showed that anodic tDCS can also improve selective attention 15. Also, tDCS application over time improved motor skill learning with a paretic upper limb and resulted in prolonged shaping of brain activation, which supported behavioral enhancements in stroke patients 16. Also, dual-tDCS increased the motor control of precision grip and digital dexterity 9. Tanaka and colleagues indicated that a single session of tDCS transiently increased knee extensor force in patients with hemi-paretic stroke 10. Furthermore, two studies distinguished that tDCS application can potentially enhance the usefulness of gait training in chronic stroke patients 18. Our study herein presents data that is in accordance to these previous studies.
Also, the advantages of tDCS on movement training has been demonstrated in many studies. In a pilot study, tDCS combined with robot-assisted gait training led to positive changes in chronic stroke 1817. Other studies have shown that the combination of bihemispheric tDCS and peripheral sensorimotor activities improved motor functions 11, motor sequence task and reaction time in patients with chronic stroke 12131419. On the other hand, our results show that anodic tDCS improved Beck Test scores. In accordance with our study, others have indeed shown that anodic tDCS has a beneficial impact on stroke.
Based on the results of the study herein and the other aforementioned studies, we demonstrate that although the use of tDCS has been recent in the treatment of neurological diseases, such as stroke, this method is promising and warrants further investigations. It seems that the increasing use of this method and its cost-effectiveness will have significant impacts on reducing the cost of treatment. Other benefits of this method, such as ease of use and very high safety in patients, are also other positive aspects of using tDCS to reduce the disabilities for people with stroke.
Conclusion
Our results demonstrate that anodic tDCS is a beneficial and safe method for increasing the rehabilitation of movement and life–related functions in chronic stroke patients, while cathodic tDCS can enhance executive memory. The ability of anodic tDCS to modulate cortical excitability becomes useful, and exploring the preference indication of the anodic and cathodic tDCS abilities requires further investigation.
One of the limitations of this study was the number of patients needed to conduct the research trial, which took a lot of research time. Among other constraints/factors were the predictable high cost, and the provision of help and assistance from various agencies, such as the Kerman Neuroscience Research Center, Kerman, Iran and Kavoush Research Center for Behavioral, Cognitive and Addiction, Guilan University of Medical Sciences, Rasht, Iran. Moreover, while the introduction of the tDCS method for patients and neurologists has garnered greater attention, more research is necessary to fully explore the advantages of this method.
Competing Interests
The authors declare no conflict of interest.
Authors' Contributions
IA: writing and critical review
KN: supervisor, writing
MA: data collection and data analysis
SAH: study design, doing experiments
SH: data collection
Acknowledgments
This work was supported by Kerman Neuroscience Research Center, Kerman, Iran and Kavoush Research Center for Behavioral, Cognitive and Addiction, Guilan University of Medical Sciences, Rasht, Iran. Also, we thanks the Prof. Vahid Sheibani, Dr. Mohammad Shabani for those kindness, assistance and considerations (Ethics code number: IR.KMU.REC.1395.23).
References
-
Hosseinzadeh
S. A..
Periferal administration of carbenoxolen reduces ischemic reperfusion injury in transient model of cerebral ischemia. Journal of Stroke and Cerebrovascular Diseases.
2008;
ooo
:
1-5
.
View Article PubMed Google Scholar -
Hosseinzadeh
S. A..
Effect of central microinjection of carbenoaolone in an experimental model of focal cerebral ischemia. Pakistan Journal of Pharmaceutical Sciences.
2009;
ooo
:
22
.
PubMed Google Scholar -
Sunwoo
H.,
Kim
Y. H.,
Chang
W. H.,
Noh
S.,
Kim
E. J.,
Ko
M. H..
Effects of dual transcranial direct current stimulation on post-stroke unilateral visuospatial neglect. Neuroscience Letters.
2013;
554
:
94-8
.
View Article PubMed Google Scholar -
Bastani
A..
Anodal transcraninal pulsed current stimulation : A novel technique to enhance corticospinal excitability. clinical. Neurophysiology.
2014;
124
:
344-51
.
-
Alexopoulos
G. S.,
Meyers
B. S.,
Young
R. C.,
Campbell
S.,
Silbersweig
D.,
Charlson
M..
Vascular depression hypothesis. Archives of General Psychiatry.
1997;
54
:
915-22
.
View Article PubMed Google Scholar -
Krishnan
K. R.,
Hays
J. C.,
Blazer
D. G..
MRI-defined vascular depression. The American Journal of Psychiatry.
1997;
154
:
497-501
.
View Article Google Scholar -
Butler
A. J.,
Shuster
M.,
O\'Hara
E.,
Hurley
K.,
Middlebrooks
D.,
Guilkey
K..
A meta-analysis of the efficacy of anodal transcranial direct current stimulation for upper limb motor recovery in stroke survivors. Journal of Hand Therapy.
2013;
26
:
162-70
.
View Article Google Scholar -
Lefebvre
S.,
P.
Laloux,
A.
Peeters,
P.
Desfontaines,
J.
Jamart,
Y.
Vandermeeren.
Dual-tDCS Enhances Online Motor Skill Learning and Long-Term Retention in Chronic Stroke Patients. Frontiers in Human Neuroscience.
2013;
6
:
343
.
View Article PubMed Google Scholar -
Lefebvre
S.,
Thonnard
J. L.,
Laloux
P.,
Peeters
A.,
Jamart
J.,
Vandermeeren
Y..
Single session of dual-tDCS transiently improves precision grip and dexterity of the paretic hand after stroke. Neurorehabilitation and Neural Repair.
2014;
28
:
100-10
.
View Article Google Scholar -
Tanaka
S.,
Takeda
K.,
Otaka
Y.,
Kita
K.,
Osu
R.,
Honda
M..
Single session of transcranial direct current stimulation transiently increases knee extensor force in patients with hemiparetic stroke. Neurorehabilitation and Neural Repair.
2011;
25
:
565-9
.
View Article Google Scholar -
Lindenberg
R.,
Renga
V.,
Zhu
L. L.,
Nair
D.,
Schlaug
G..
Bihemispheric brain stimulation facilitates motor recovery in chronic stroke patients. Neurology.
2010;
75
:
2176-84
.
View Article PubMed Google Scholar -
Celnik
P.,
Paik
N. J.,
Vandermeeren
Y.,
Dimyan
M.,
Cohen
L. G..
Effects of combined peripheral nerve stimulation and brain polarization on performance of a motor sequence task after chronic stroke. Stroke.
2009;
40
:
1764-71
.
View Article Google Scholar -
Boggio
P. S.,
Nunes
A.,
Rigonatti
S. P.,
Nitsche
M. A.,
Pascual-Leone
A.,
Fregni
F..
Repeated sessions of noninvasive brain DC stimulation is associated with motor function improvement in stroke patients. Restorative Neurology and Neuroscience.
2007;
25
:
123-9
.
PubMed Google Scholar -
Hummel
F.,
Celnik
P.,
Giraux
P.,
Floel
A.,
Wu
W. H.,
Gerloff
C..
Effects of non-invasive cortical stimulation on skilled motor function in chronic stroke. Brain.
2005;
128
:
490-9
.
View Article PubMed Google Scholar -
Au-Yeung
S. S.,
Wang
J.,
Chen
Y.,
Chua
E..
Transcranial direct current stimulation to primary motor area improves hand dexterity and selective attention in chronic stroke. American Journal of Physical Medicine & Rehabilitation.
2014;
93
:
1057-64
.
View Article PubMed Google Scholar -
Lefebvre
S.,
Dricot
L.,
Laloux
P.,
Gradkowski
W.,
Desfontaines
P.,
Evrard
F..
Neural substrates underlying stimulation-enhanced motor skill learning after stroke. Brain.
2015;
138
:
149-63
.
View Article PubMed Google Scholar -
Viana
R. T.,
Laurentino
G. E.,
Souza
R. J.,
Fonseca
J. B.,
Filho
E. M. Silva,
Dias
S. N..
Effects of the addition of transcranial direct current stimulation to virtual reality therapy after stroke: a pilot randomized controlled trial. NeuroRehabilitation.
2014;
34
:
437-46
.
PubMed Google Scholar -
Geroin
C.,
Picelli
A.,
Munari
D.,
Waldner
A.,
Tomelleri
C.,
Smania
N..
Combined transcranial direct current stimulation and robot-assisted gait training in patients with chronic stroke: a preliminary comparison. Clinical Rehabilitation.
2011;
25
:
537-48
.
View Article PubMed Google Scholar -
Hummel
F.,
Cohen
L. G..
Improvement of motor function with noninvasive cortical stimulation in a patient with chronic stroke. Neurorehabilitation and Neural Repair.
2005;
19
:
14-9
.
View Article PubMed Google Scholar
Comments
Downloads
Article Details
Volume & Issue : Vol 5 No 11 (2018)
Page No.: 2841-2849
Published on: 2018-11-30
Citations
Copyrights & License
This work is licensed under a Creative Commons Attribution 4.0 International License.
Search Panel
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Search for this article in:
Google Scholar
Researchgate
- HTML viewed - 7762 times
- Download PDF downloaded - 2195 times
- View Article downloaded - 0 times
