

Copyrights: Jahnavi Reddy Yeduguri, Kalyani Raju, Abhay Khattepur, Nethra Nattiala, Nithya Shree Balaji, Pooja B Kolkar, 2024. License: This work is licensed under a Creative Commons Attribution 4.0 International License.
Abstract
Introduction: Pleomorphic liposarcoma is one of the rarest malignancies. In this case report, we present a primary pleomorphic liposarcoma of the retroperitoneal cavity in a 73-year-old male patient.
Case Presentation: Contrast-enhanced computed tomography revealed a giant mass in the right abdomen (retroperitoneal) with areas of fat attenuation, appearing to encase the right kidney and showing features of a retroperitoneal liposarcoma involving the right kidney. The patient subsequently underwent surgery, and the specimen sent for histopathological examination was confirmed as pleomorphic liposarcoma of the retroperitoneal cavity. Additionally, papillary thyroid carcinoma, which is usually seen in younger patients and rarely presents as part of synchronous malignancies, was noted in this case where the same patient presented with a swelling in the front of the neck. Fine needle aspiration cytology revealed it to be papillary thyroid carcinoma. Following surgery, histopathological examination of the specimen confirmed it as a papillary variant of thyroid carcinoma.
Conclusion: This case report highlights the occurrence of rare synchronous malignancies of both epithelial and non-epithelial/sarcomatous origin. The concurrent presentation of papillary thyroid carcinoma with pleomorphic liposarcoma is particularly rare.
Introduction
Synchronous tumors are malignancies that are diagnosed within 6 months of the diagnosis of the primary tumor1. Liposarcoma is one of the most common malignant tumors of soft tissues, accounting for up to 20% of all adult mesenchymal neoplasms1. It generally has a poor prognosis and frequently metastasizes to the lungs, followed by the spine and liver2, 3. Recent data categorize liposarcoma into three major groups: well-differentiated liposarcoma, dedifferentiated liposarcoma, atypical lipomatous tumors, myxoid variant, and pleomorphic variant of liposarcoma2, 4. The solid variant of papillary thyroid carcinoma is one of the rarest forms and is usually seen in young adults with prior exposure to ionizing radiation5. The treatment strategies for both malignancies are similar, as R0 resection represents the treatment of choice5, 6. Recent case studies have shown an increased incidence of patients with Hashimoto’s thyroiditis along with thyroid carcinoma. In this case report, we describe a patient presenting with pleomorphic liposarcoma encasing the kidney, accompanied by papillary thyroid carcinoma with Hashimoto’s thyroiditis5, 6.
Case Report
A 73-year-old male patient from the southern part of Karnataka presented with complaints of severe abdominal distension for the past 3 weeks to a tertiary healthcare hospital. The patient's past medical and surgical history was not relevant to the case. Upon examination, a mass measuring 45 x 30 x 20 cm was found below the right costal margin, without tenderness. All blood tests, including a complete blood picture, were within the normal range. Biochemical parameters, including liver function tests, thyroid function tests, and renal function tests, did not reveal anything significant. Contrast-enhanced computed tomography (CECT) showed a giant mass in the right abdomen (retroperitoneal) with areas of fat attenuation, appearing to encase the right kidney and showing features of retroperitoneal liposarcoma involving the right kidney (Figure 1). The patient underwent complete resection of the retroperitoneal mass along with right nephrectomy and R0 resection, and the specimen was subjected to histopathological examination. Additionally, this case report emphasizes potential insights into the etiology, diagnosis, treatment strategies, and multidisciplinary approaches for patients presenting with multiple malignancies. The follow-up for this patient was lost.



Gross Findings
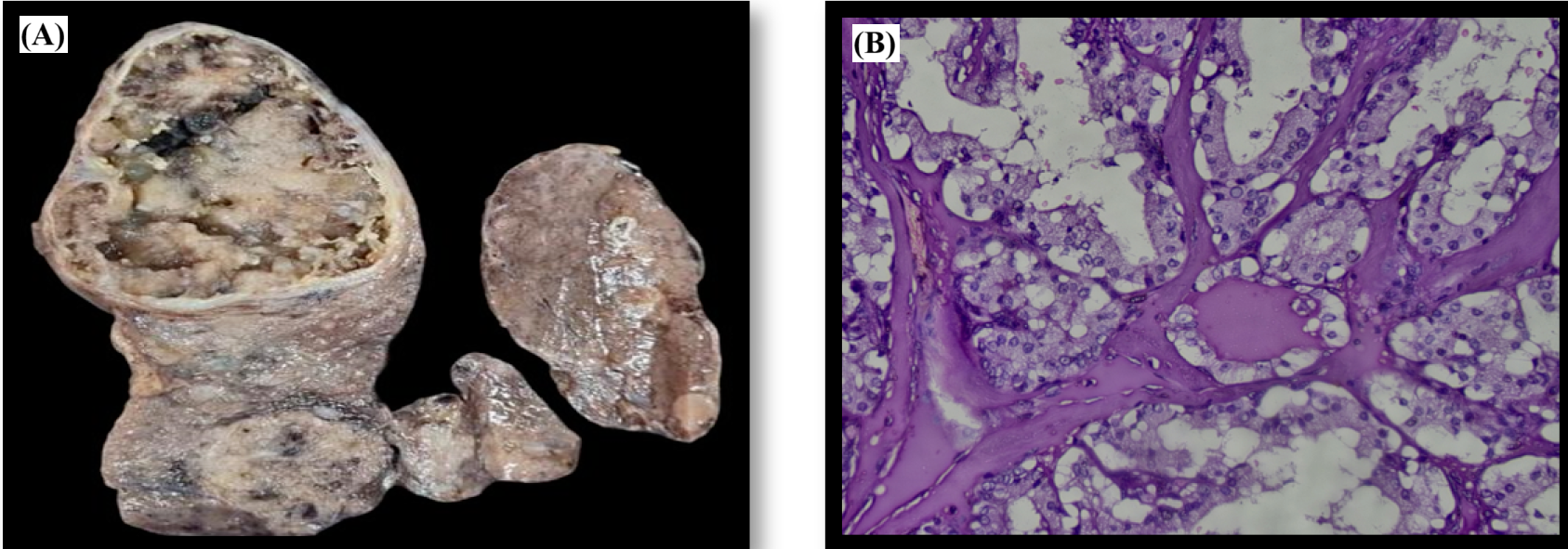
The gross examination revealed a grey-yellow to grey-brown soft tissue mass weighing 12 kg and measuring 42 x 33 x 23 cm. The right kidney, measuring 6 x 4.5 x 4 cm, appeared to be encased by the tumor, and the renal capsule could not be separated from the mass (Figure 2a).
Microscopic Findings
Microscopy showed sheets of pleomorphic lipoblasts with cytoplasmic lipid vacuoles and enlarged, scalloped, hyperchromatic nuclei. Among these were noted spindle cells with tapering ends and pleomorphic nuclei. Myxoid areas were also observed. Features of pleomorphic liposarcoma were confirmed on histopathology (Figure 2b).
Two weeks later, the patient presented with cervical lymphadenopathy, and on clinical examination, an enlarged thyroid gland was noted. Subsequently, the patient underwent fine needle aspiration cytology of the thyroid and was diagnosed with papillary carcinoma of the thyroid. The patient then underwent total thyroidectomy with central node dissection and bilateral selective neck dissection, and the specimen was subjected to histopathological examination.
Gross Findings
The gross examination of the total thyroidectomy specimen measured 10 x 7.5 x 3.5 cm. The right thyroid measured 10 x 4.5 x 3.5 cm, the isthmus measured 2 x 2 x 1 cm, and the left thyroid measured 5 x 3 x 1 cm. The cut surface of the right thyroid showed a well-circumscribed lesion with grey-brown to grey-black papillary excrescences at the superior pole measuring 4.5 x 3.5 x 2 cm and another circumscribed grey-white lesion at the inferior pole measuring 2.4 x 1.5 cm. The cut surface of the left thyroid showed a grey-white area near the lateral inferior lobe measuring 1.5 x 1 x 0.5 cm (Figure 3a).
Microscopic Findings
Microscopy showed tumor cells arranged in a papillary pattern with a fibrovascular core and areas of hyalinization. Individual tumor cells were cuboidal with scant eosinophilic cytoplasm, showing nuclear pleomorphism with an increased nuclear-cytoplasmic ratio, oval nuclei with a ground glass appearance, and nuclear grooves. These tumor cells were infiltrating the capsule. Focal areas displayed Hashimoto's thyroiditis with Hurthle cell change (Figure 3b).
Discussion
Pleomorphic liposarcoma is commonly characterized by the growth of a large, painless tumor, typically presenting as a huge mass or with compression symptoms due to its large size2. Pleomorphic liposarcoma is most often seen in the lower extremities, especially the proximal part, and is rarely observed in the retroperitoneal region2, 3. Radiological investigations such as Ultrasound, Computed Tomography (CT), and Magnetic Resonance Imaging (MRI) are essential for assessing the size of the tumor, the extent of the tumor, and the degree of infiltration into surrounding structures2, 3. The final diagnosis of pleomorphic liposarcoma relies heavily on histopathological examination, which reveals pleomorphic lipoblasts with vacuoles in the cytoplasm, intensely stained nuclei, and large nucleoli, along with spindle cells3. Surgical resection is the treatment of choice, and palliative treatment is also provided for those patients with recurrence or metastasis and to relieve compression symptoms2, 3, 4.
On the other hand, the papillary variant of thyroid malignancies has a good prognosis and a lower rate of recurrence compared to other malignancies.5 Recent studies have shown that in cases with clinically insignificant carcinoma of the thyroid, abnormal iodine levels, radiation exposure, and nutrition are the most important factors associated with it5, 6. The association of papillary thyroid carcinoma with Hashimoto's thyroiditis has been noted several times6. Total thyroidectomy with neck node dissection is the treatment of choice, whereas some patients may require radioiodine therapy if an associated goiter is noted6. Microscopically, papillary thyroid carcinoma typically presents in a papillary architecture with papillary fronds surrounding a fibrovascular core. The individual nuclei show characteristic clearing and nuclear grooves5, 6.
A study conducted by Hao L suggests that the presentation of patients with multiple malignancies allows us to consider the possibilities in understanding the etiology of human cancer and proposes new mechanisms and hypotheses for carcinogenesis1. This also emphasizes the importance of genetic testing, including oncogenes, for cancer susceptibility in individuals1.
Conclusion
This case report highlights the occurrence of rare synchronous malignancies of both epithelial and non-epithelial/sarcomatous origin. The concurrent presentation of papillary thyroid carcinoma with pleomorphic liposarcoma is particularly rare. Furthermore, this report underscores the role of oncogenes in precipitating multiple malignancies, their progression, and metastasis. The importance of complete surgical resection and targeted curative therapy within a patient-centered multidisciplinary approach offers the best strategy for improved patient care and cure. Regular follow-ups with clinical examinations and radiological investigations such as ultrasound, CT, and MRI are crucial for monitoring disease progression, assessing metastatic status, and facilitating the early diagnosis of primary cancer. Genetic analysis of this patient could not be conducted, and follow-up with this patient was lost.
Abbreviations
CECT - Contrast-Enhanced Computed Tomography, CT - Computed Tomography, MRI - Magnetic Resonance Imaging
Acknowledgments
None.
Author’s contributions
JRY: Data collection, drafting the manuscript, photographs; KR: Concept, manuscript review and editing; AK: Surgical oncologist who operated the case; NN: Data collection, drafting the manuscript; NSB: Data collection, drafting the manuscript; PBK: Data collection, drafting the manuscript. All authors read and approved the final manuscript.
Funding
None.
Availability of data and materials
Data and materials used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics approval and consent to participate
The consent from the patient has been taken. The ethics clearance has been taken from the Institute Ethics Committee.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Competing interests
The authors declare that they have no competing interests.
References
-
Hao
L.,
Zhang
L.,
Xu
C.,
Jiang
M.,
Zhu
G.,
Guo
J.,
Multiple synchronous primary malignant neoplasms: A case report and literature review. Oncology Letters.
2023;
26
(4)
:
1-7
.
View Article Google Scholar -
Amer
K.M.,
Congiusta
D.V.,
Thomson
J.E.,
Elsamna
S.,
Chaudhry
I.,
Bozzo
A.,
Epidemiology and survival of liposarcoma and its subtypes: A dual database analysis. Journal of Clinical Orthopaedics and Trauma.
2020;
11
:
479-84
.
View Article Google Scholar -
Torigoe
T.,
Matsumoto
T.,
Terakado
A.,
Takase
M.,
Yamasaki
S.,
Kurosawa
H.,
Primary pleomorphic liposarcoma of bone: MRI findings and review of the literature. Skeletal Radiology.
2006;
35
(7)
:
536-8
.
View Article Google Scholar -
Macmull
S.,
Atkinson
H.D.,
Saso
S.,
Tirabosco
R.,
O'Donnell
P.,
Skinner
J.A.,
Primary intra-osseous liposarcoma of the femur: a case report. Journal of Orthopaedic Surgery (Hong Kong).
2009;
17
(3)
:
374-8
.
View Article Google Scholar -
Fulciniti
F.,
Barizzi
J.,
Trimboli
P.,
Giovanella
L.,
Solid papillary thyroid carcinoma with Hashimoto's thyroiditis: description of a further case with challenging cytological features. BMJ Case Reports.
2019;
12
(1)
:
34-8
.
View Article Google Scholar -
Mahuli
K.,
Mahakalkar
C.,
Jajoo
S.,
Chava
A.,
Kantode
V.,
Wanjari
M.,
A rare case of papillary thyroid carcinoma (PTC) presenting as multinodular goitre (MNG) successfully operated with total thyroidectomy (TT). Medical Science.
2022;
26
:
ms533e2551
.
View Article Google Scholar
Comments
Article Details
Volume & Issue : Vol 11 No 8 (2024)
Page No.: 6661-6665
Published on: 2024-08-31
Citations
Copyrights & License
This work is licensed under a Creative Commons Attribution 4.0 International License.
Search Panel
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Search for this article in:
Google Scholar
Researchgate
- HTML viewed - 1796 times
- PDF downloaded - 715 times
- XML downloaded - 76 times
