

Copyrights: Hung Van Nguyen, Thanh Tuan Nguyen, Chuong Van Tran, Luan Thi Dao, 2024. License: This work is licensed under a Creative Commons Attribution 4.0 International License.
Abstract
Introduction: Predicting the node status of stomach carcinoma is very useful, as it affects treatment decisions. The objective of this study was to use the immunohistochemical expression of E-cadherin and tumor budding to investigate the nodal status of gastric cancer surgical specimens as a pilot study before application to gastric cancer biopsy samples.
Methods: Three hundred and eleven (311) gastric cancer surgical samples with lymph node dissection were retrospectively evaluated at Hanoi Medical University Hospital, Vietnam. The comparison of tumor budding and E-cadherin expression with lymph node status was investigated. Tumor budding was calculated on the microfield of 0.785 mm2 according to the 2016 International Consensus Conference guidelines. The immunoexpression of the E-Cadherin protein was examined by immunohistochemistry.
Results: The overall lymph node metastasis rate was 55.6%. In multivariable logistic regression analyses, tumor budding (odds ratio [OR] = 12.73, 95% confidence interval [CI] = 4.980–32.53, p < 0.001), immunoexpression of E-cadherin (OR = 0.048, 95% CI = 0.019–0.121, p < 0.001), stage (OR = 2.329, 95% CI = 1.204–4.504, p = 0.012), and grade (OR = 2.032, 95% CI = 1.081–3.820, p = 0.028) were critical factors that can independently predict lymph node status.
Conclusions: Tumor budding and E-cadherin expression are independent factors and may be additional candidates in predicting node status in patients with primary gastric carcinoma.
Introduction
Gastric adenocarcinoma accounts for about 90% of stomach carcinoma cases. Morbidity and mortality due to stomach cancer are much higher in Southeast Asian countries than in others worldwide1. The depth of microscopic invasion is usually proportional to the rate of lymph node metastasis, with pT1 being 2.3%, pT2 at 21.9%, pT3 at 64.2%, and pT4 at 86.6%2. Lymph node metastasis may be present in 3%–20% of early gastric cancer cases3, 4. According to GLOBOCAN data in 2020, gastric cancer ranks third in both new cases and deaths in Vietnam, with a male-to-female ratio of about 2.3:15.
Numerous factors may be related to the prognosis of stomach cancer, including histological grade, histological type, tumor spread, the number of lymph nodes involved, and pT and pN stage. However, the most challenging task is identifying lymph node metastases because the nodes of the stomach are numerous and located deep in the abdomen, and non-invasive methods to detect lymph node metastases have limited accuracy6, 7, 8, 9, 10, 11, 12. Due to the numerous lymph nodes involved in stomach carcinoma being localized in unfavorable locations for biopsy, it is not possible to perform a biopsy of all these suspected metastatic nodes. Therefore, a more detailed study of the histopathological characteristics of the primary tumor to find clues that can predict lymph node metastasis is necessary. Several histological features of the primary tumor may be indicative of lymph node metastasis, including lymphatic invasion, Lauren subtype, tumor budding, and E-cadherin expression; however, these were not used in the assessment of lymph node status by previous works11, 13. Two of these, including tumor budding and E-cadherin expression, have been mentioned in this work in relation to lymph node metastasis.
By definition, tumor budding is a single cell or a small group of 2-4 tumor cells in the invasive area of the tumor11. High-grade tumor budding is considered a poor prognostic factor for numerous cancers such as colorectal cancer, breast cancer, pancreatic cancer, and squamous cell carcinoma of the head and neck11. Increased tumor budding and suppression of E-cadherin immunoexpression are indicative of epithelial-mesenchymal transformation (EMT), a critical process of cancer metastasis14, 15. The E-cadherin protein binds epithelial cells together and maintains their polarity. In carcinoma, cancer cells easily separate from the original tumor (the first step in metastasis) because their reduced E-cadherin expression causes them to lose their polarity. Cancer cells' EMT enables them to migrate and metastasize more easily to distant sites. The objective of this study was to evaluate the ability to predict nodal status using tumor budding and E-cadherin immunoexpression of primary gastric adenocarcinoma on surgical specimens as a pilot study before application to gastric cancer biopsy samples.
Methods
Data Collection and Research Parameters
The retrospective study included 311 patients with primary gastric cancer undergoing surgery for the first time, all of whom had lymph node dissection at Hanoi Medical University Hospital, Vietnam, between October 2019 and June 2021. Patients with recurrent or secondary gastric cancer were not included in this study. The patients in this study were all from the Northern region of Vietnam. Retrospective data on imaging studies, such as scintigraphy or histopathological evaluation of surgical tumor specimens with or without accompanying metastatic specimens, were used to evaluate distant metastases. This study received permission from the Ethics Committee of Hanoi Medical University (decision number: 4397/QD-DHYHN), complies with the ethical standards set forth in the Declaration of Helsinki, and was revised by the World Medical Association’s General Assembly in Seoul, South Korea, in October 2008.
Data on patient age, gender, lymph node status, distant metastasis, histological type, and primary tumor location were obtained from digitized archival records. H&E-stained slides and corresponding tissue samples enclosed in paraffin blocks were also obtained to study E-Cadherin expression. Histological gastric carcinoma variants were identified based on the 2019 World Health Organization (WHO) histological classification of gastrointestinal cancer1. The tumors’ pT and pN classifications were determined using the eighth edition of the American Joint Committee on Cancer classification system1.
Tumor budding was evaluated using the International Tumor Budding Consensus Conference (ITBCC) 2016 protocol11. Tumor budding was counted in the “hotspot” field (tumor tissue areas with the most tumor buds) at 20× magnification (corresponding to an evaluation area of 0.785mm²). The “hotspot” areas are usually at the edge of the tumor. Ten microscopic fields at invasive areas were scanned at 10× magnification to identify “hotspot” areas. Two pathologists counted the tumor buds in the “hotspot” areas at 20× magnification. The number of tumor buds was calculated by counting in the "hotspot" field and then dividing by the conversion factor to determine the number of tumor buds/0.785 mm². Tumor budding was graded as low (0–4 tumor buds/0.785 mm²), moderate (5–9 tumor buds/0.785 mm²), and high (≥ 10 tumor buds/0.785 mm²). Differences in tumor budding grades between the two pathologists were discussed and re-evaluated.
Immunohistochemistry
After the steps of routine microscopic techniques, immunostaining was performed using a Ventana Benchmark XT automatic stainer and an anti-E-cadherin (mouse monoclonal primary antibody) antibody kit (cat. no.: 760-500/05269806001; diagnostics Roche, USA). Two pathologists, blind to the cases’ clinical data, semi-quantitatively analyzed the E-cadherin staining results for gastric adenocarcinoma tissue samples from 311 cases. The cellular membrane is the main location of E-cadherin immunoexpression, and sometimes this expression extends into the cytoplasm. In each tumor, the rate of immunostained cells was determined by counting 500 tumor cells. Scoring of E-cadherin expression is based on immunostaining intensity (0=negative; 1=low; 2=moderate; 3=strong) and the percentage of immunoreactive cells (0=none; 1=1%–9%; 2=10%–49%; 3=50%–79%; 4=80%–100%) and grading: 0=negative score; 1+ =score of 1–4; 2+ =score of 5–8; 3+ =score of 9–1216.
Analyzed Parameters and Relationships
E-cadherin expression and tumor budding were analyzed relative to several clinical pathological parameters: histopathological type (WHO and Lauren’s classification), grade, lymph node metastasis, stage pT, age, and sex. E-cadherin expression was classified as low (0–1+) and high (2+–3+). Tumor budding was classified as low grade (0–4 tumor buds/0.785mm²) and high grade (≥5 tumor buds/0.785mm²). In E-cadherin expression, the original group was named “EcadhGOC”, consisting of 4 levels: 0, 1+, 2+, and 3+; we regrouped them into low (0–1+) and high (2+–3+) titled “phanlopE1”. Similarly, in tumor budding, the original group was named “Budding”, consisting of 3 levels: low (0–1+), medium (2+), and high (3+); we regrouped them into low (0–1+) and high (2+–3+) titled “phanlopB2”. For the purpose of comparing the predictability of lymph node status of the respective groups, the receiver-operating characteristic (ROC) curve was used in the analysis.
Statistical Analysis
SPSS 20 for Windows software (SPSS, Inc., Chicago, IL, USA) was used to analyze the data. The χ² test was used to compare proportions, and Fisher's exact test was used for cases with expected frequencies < 5. The associations of various variables with a binary dependent variable were determined using multivariable logistic regression analysis. Statistical significance was determined when the difference was p < 0.05. The receiver-operating characteristic curve (ROC) and the area under the curve (AUC) were used to investigate the ability of two parameters to predict lymph node metastasis, including tumor budding and E-cadherin expression. Good predictability is indicated when the AUC is ≥ 0.8.
| Clinicopathologic features | Total n = 311 (100%) | |
| n (%) | ||
| Ages | ||
| 40-49 | 24 (7.7%) | |
| 50-59 | 81 (26%) | |
| 60-69 | 144 (46.3%) | |
| 70-79 | ||
| 80-89 | 6 (1.9%) | |
| Sex | ||
| Nam | 203 (65.3%) | |
| Nữ | 108 (34.7%) | |
| Lauren's histological type | ||
| Intestinal | 211 (67.8%) | |
| Mixed | 52 (16.7%) | |
| Diffuse | 48 (15.4%) | |
| WHO histological type | ||
| Tubular | 206 (66.2%) | |
| Poorly cohesive | 50 (16.1%) | |
| Mucinous | 3 (1%) | |
| Mixed | 51 (16.4%) | |
| With lymphoid stroma | 1 (0.3%) | |
| Grade (WHO) | ||
| High | 142 (45.7%) | |
| Moderate | 93 (29.9%) | |
| Poor | 76 (24.4%) | |
| Stage | ||
| T1a | 3 (1%) | |
| T1b | 13 (4.2%) | |
| T2 | 54 (17.4%) | |
| T3 | 217 (69.8%) | |
| T4a | 20 (6.4%) | |
| T4b | 4 (1.3%) | |
| Lymph nodes metastasis | ||
| Yes | 173 (55.6%) | |
| No | 138 (44.4%) | |
| E-Cadherin expression | ||
| Weak | 136 (43.7%) | |
| Strong | 175 (56.3%) | |
| Tumor budding | ||
| Low | 108 (34.7%) | |
| High | 203 (65.3%) | |
| Clinicopathologic parameters | Lymph nodes metastasis | |||
| No | Yes | p | ||
| Ages | ||||
| 40-49 | 9 | 15 | 0.470 | |
| 50-59 | 41 | 40 | ||
| 60-69 | 65 | 79 | ||
| 70-79 | 20 | 36 | ||
| 80-89 | 3 | 3 | ||
| Sex | ||||
| Nam | 81 | 122 | 0.030 | |
| Nữ | 57 | 51 | ||
| Lauren's histological type | ||||
| Intestinal | 126 | 85 | <0.001 | |
| Mixed | 9 | 43 | ||
| Diffuse | 3 | 45 | ||
| WHO histological type | ||||
| Tubular | 124 | 82 | <0.001 | |
| Poorly cohesive | 3 | 47 | ||
| Mucinous | 0 | 3 | ||
| Mixed | 10 | 41 | ||
| With lymphoid stroma | 1 | 0 | ||
| Grade (WHO) | ||||
| High | 100 | 42 | <0.001 | |
| Moderate | 35 | 58 | ||
| Poor | 3 | 73 | ||
| Stage | ||||
| T1a | 3 | 0 | <0.001 | |
| T1b | 10 | 3 | ||
| T2 | 41 | 13 | ||
| T3 | 83 | 134 | ||
| T4a | 1 | 19 | ||
| T4b | 0 | 4 | ||
| E-Cadherin expression | ||||
| Weak | 10 | 126 | <0.001 | |
| Strong | 128 | 47 | ||
| Tumor budding | ||||
| Low | 96 | 12 | <0.001 | |
| High | 42 | 161 | ||
| Clinicopathologic parameters | Lymph nodes metastasis | ||||||
| No | Yes | OR | 95%CI | p | |||
| Lauren's histological type | |||||||
| Intestinal | 126 | 85 | 2.067 | 1.125-3.799 | 0.019 | ||
| Mixed | 9 | 43 | |||||
| Diffuse | 3 | 45 | |||||
| Stage | |||||||
| T1a | 3 | 0 | 2.233 | 1.165-4.281 | 0.016 | ||
| T1b | 10 | 3 | |||||
| T2 | 41 | 13 | |||||
| T3 | 83 | 134 | |||||
| T4a | 1 | 19 | |||||
| T4b | 0 | 4 | |||||
| E-Cadherin expression | |||||||
| Weak | 10 | 126 | 0.043 | 0.017-0.108 | <0.001 | ||
| Strong | 128 | 47 | |||||
| Tumor budding | |||||||
| Low | 96 | 12 | 14.59 | 5.895-36.09 | <0.001 | ||
| High | 42 | 161 | |||||
| Clinicopathologic parameters | Lymph nodes metastasis | |||||
| No | Yes | OR | 95%CI | p | ||
| WHO histological type | ||||||
| Tubular | 124 | 82 | 1.028 | 0.722-1.463 | 0.879 | |
| Poorly cohesive | 3 | 47 | ||||
| Mucinous | 0 | 3 | ||||
| Mixed | 10 | 41 | ||||
| With lymphoid stroma | 1 | 0 | ||||
| Grade (WHO) | ||||||
| High | 100 | 42 | 2.032 | 1.081-3.820 | 0.028 | |
| Moderate | 35 | 58 | ||||
| Poor | 3 | 73 | ||||
| Stage | ||||||
| T1a | 3 | 0 | 2.329 | 1.204-4.504 | 0.012 | |
| T1b | 10 | 3 | ||||
| T2 | 41 | 13 | ||||
| T3 | 83 | 134 | ||||
| T4a | 1 | 19 | ||||
| T4b | 0 | 4 | ||||
| E-Cadherin expression | ||||||
| Weak | 10 | 126 | 0.048 | 0.019-0.121 | <0.001 | |
| Strong | 128 | 47 | ||||
| Tumor budding | ||||||
| Low | 96 | 12 | 12.73 | 4.980-32.53 | <0.001 | |
| High | 42 | 161 | ||||




Results
The average age of the 311 patients in this study was 62.99 ± 8.64 years (with an age range of 42–85 years), and the male/female ratio was 1.9/1. Most cases belonged to pT3 (69.8%), followed by pT2 (17.4%), pT4 (7.7%), and pT1 (5.1%). The overall node metastasis rate was 55.6%. Incidence of node metastasis was 18.7% for pT1, 25.9% for pT2, 47.0% for pT3, and 91.7% for pT4. The number of nodes dissected in each case ranged from 0 to 28. The patient's clinical-pathological manifestations are summarized in Table 1.
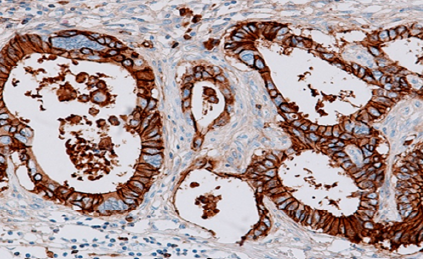
Univariate analysis (Table 2) found lymph node metastasis associated with many parameters: sex (p = 0.001), Lauren’s histological type (p < 0.001), WHO histological type (p < 0.001), WHO histological grade (p < 0.001), pT stage (p < 0.001), tumor budding (p < 0.001), and E-cadherin expression (p < 0.001). However, it was not involved in age (p = 0.408). Among the 173 (55.6%) cases with node metastasis, tumor budding (Figure 1) was 3+ (high) in 79.3% (161/203) and 1+ (low) in 11.1% (12/108; p<0.001). Similarly, E-cadherin immunoexpression (Figure 2) was weak in 92.6% (126/136) and strong in 26.8% (47/175; p < 0.001).
Through multivariate logistic regression analysis, tumor budding (odds ratio [OR] = 14.59, 95% confidence interval [CI] = 5.89–36.09, p < 0.001), E-cadherin expression (OR = 0.043, 95% CI = 0.017–0.108, p < 0.001), stage (OR = 2.233, 95% CI = 1.165–4.281, p = 0.016), and Lauren type (OR = 2.067, 95% CI = 1.125–3.799, p = 0.019) were independent factors of lymph node metastasis in the Lauren histology group (Table 3).
In the WHO histological group, multivariate logistic regression analysis identified tumor budding (OR=12.73, 95% CI = 4.980–32.530, p < 0.001), E-cadherin expression (OR=0.048, 95% CI=0.019–0.121, p < 0.001), stage (OR = 2.329, 95% CI = 1.204–4.504, p = 0.012), and grade (OR = 2.032, 95% CI = 1.081–3.820, p = 0.028) as independent factors of lymph node metastasis (Table 4).
In terms of tumor budding, the AUC=0.89 (95% CI: 0.85-0.93, p < 0.001) in the original group (budding) and AUC=0.81 (95% CI: 0.76-0.87, p < 0.001) in the regrouped tumor budding (phanlopB2) both revealed high prognostic ability for node metastasis (Figure 3). For E-cadherin immunoexpression, the AUC=0.87 (95% CI: 0.83-0.91, p<0.001) in the original group (EcadhGOC) and the AUC=0.83 (95% CI: 0.78-0.88, p<0.001) in regrouped E-cadherin expression (phanlopE1) both showed a high predictive ability of lymph node metastasis (Figure 4).
Discussion
The rate of node metastasis in stomach cancer patients increased with pT stage in our study. Many other works have also found that the more advanced the gastric cancer, the deeper the invasion and the higher the rate of node metastasis17, 18, 19. The association of node metastasis with tumor budding and E-cadherin immunoexpression was confirmed by univariate analysis (Table 2). EMT of tumor cells may be the cause of these phenomena. EMT has been involved in the metastasis of stomach cancer and many other carcinomas20. This transformation has been described to downregulate E-cadherin expression (an immunomarker for epithelial cells) and upregulate vimentin expression (the mesenchymal marker)21, and be associated with increased tumor budding22. EMT may have a significant effect on the mechanism of tumor invasion, which has been suggested in some studies14, 15. Bronsert et al. have noticed that cells of tumor budding in various cancers (colorectal, pancreatic ductal carcinoma, lung adenocarcinoma, and invasive ductal breast carcinoma) had lost their polarity (more round and spindle shape), decreased E-cadherin staining intensity, decreased membrane E-cadherin staining, and increased nuclear zinc finger E-box binding homeobox 1 (ZEB1) staining23.
Human E-cadherin, a transmembrane glycoprotein mainly involved in epithelial cell adhesion, is encoded in the cadherin 1 (CDH1) gene of chromosome 16q22.124. E-cadherin binds to cytoskeleton actin to maintain cell structure stability, inhibits individual cell migration, and is involved in cell signaling25, 26. Increased abilities such as cell-cell interactions, migration, invasion, and metastasis of tumor cells are significantly influenced by aberrant E-cadherin immunoexpression27, 28.
The intensive (normal) expression rate of E-cadherin in cell membranes and cytoplasm was higher than the weak (abnormal) expression rate. Multivariate regression analysis demonstrated that E-cadherin immunoexpression is an independent factor associated with tumor grade (OR = 0.23, 95% CI = 0.12–0.43, p < 0.001), tumor budding (OR = 10.61, 95% CI = 2.73–41.16, p = 0.001), and lymph node metastasis (OR = 0.04, 95% CI = 0.012–0.134, p < 0.001). Several other studies have found abnormalities of E-cadherin immunoexpression in 25%29 or 46.7% – 48.6%30, 31 of cases and are closely related to lymph node metastasis. Several meta-analyses have suggested a significant association between E-cadherin expression and several variables, including invasion (p < 0.001), node metastasis (p < 0.001), and distant spread (p < 0.001), resulting in low five-year survival (p < 0.001)32, 33, 34, 35. Numerous studies have discovered E-cadherin as a crucial tumor suppressor in several cancers, including gastric carcinoma35, 36. One study found that 33% – 50% of incident gastric cancers had somatic E-cadherin inactivating mutations, and 63.6% of patients with signet ring cell carcinoma had decreased E-cadherin immunoexpression37. Expression dysfunction of E-cadherin is caused by multiple molecular mechanisms, for instance CDH1 mutations38, DNA hypermethylation32, and non-coding microRNAs. Reducing immunoexpression of E-cadherin at the cell membrane causes an attenuation or complete loss of cell-cell interactions and leads to the inhibition of the activation of transcription factors snail homolog 1 (SNAIL), twist family bHLH transcription factor 1 (TWIST), and ZEB1, leading to EMT33, 39. These reasons have caused differences in E-cadherin expression in different studies. CDH1 gene mutations correlate with many factors (geography, race, and especially eating habits) that are known to influence cancer risk in general.
Tumor budding should be distinguished from poorly differentiated cell clusters. A cell cluster with ≥ 5 cancer cells invading the stromal tissue and not forming glands is called poorly differentiated clusters40. The tumor budding concept has been mentioned for a long time, but only recently has it garnered interest in further research. It has been discovered that tumor budding has the potential to increase node metastasis, distant spread, tumor stage, and survival prognosis in numerous cancers, including colon cancer41, esophageal squamous carcinoma42, breast cancer43, and lung cancer44. ITBCC confirmed that tumor budding can predict the prognosis of node status in stage pT1 colorectal cancer and the survival ability of patients with stage II colorectal cancer11.
At the molecular level, the association between tumor budding and E-cadherin immunoexpression has been interpreted as tumor budding correlates with the high CpG island methylator phenotype (CIMP-H), which occurs in 40% of cancer cases. Microsatellite instability and CIMP-H cases often present with similar clinical and molecular features: tumor location, poor differentiation, and B-Raf proto-oncogene, serine/threonine kinase (BRAF) mutations45. E-cadherin loss in gastrointestinal carcinoma may be related to methylation of the O6-methylguanine-DNA methyltransferase (MGMT) promoter, which is part of the EMT pathway that induces Wnt pathway activation and nuclear beta-catenin translocation, thereby affecting E-cadherin expression41.
Conclusion
Predicting node status in stomach cancer is very useful because it affects the selection of appropriate surgical methods and treatment combinations. This study found that tumor budding and E-cadherin immunoexpression are independent factors and may be strong candidates for predicting node metastasis of primary stomach cancer based on surgical specimens. According to the conventional concepts, small biopsy samples often do not have enough necessary information such as pT stage, vascular, and nerve invasion, so predicting lymph node status using traditional methods is impossible. Therefore, this study can be considered a pilot work to predict lymph node metastasis before applying it to small biopsy samples of gastric cancer.
Abbreviations
AUC: Area Under the Curve, BRAF: B-Raf Proto-Oncogene, Serine/Threonine Kinase, CDH1: Cadherin 1, CI: Confidence Interval, CIMP-H: CpG Island Methylator Phenotype - High, EMT: Epithelial-Mesenchymal Transformation, GLOBOCAN: Global Cancer Observatory, H&E: Hematoxylin and Eosin, ITBCC: International Tumor Budding Consensus Conference, MGMT: O6-Methylguanine-DNA Methyltransferase, OR: Odds Ratio, ROC: Receiver-Operating Characteristic, SNAIL: Snail Homolog 1, SPSS: Statistical Package for the Social Sciences, TWIST: Twist Family bHLH Transcription Factor 1, WHO: World Health Organization, ZEB1: Zinc Finger E-Box Binding Homeobox 1
Acknowledgments
We would like to thank the University for the study’s approval.
Author’s contributions
NVH, NTT: Conceptualization, Methodology, Writing-Original draft preparation; NTT, TVC: Visualization, Methodology, Software; TVC, NVH, DTL: Data curation, Writing-Original draft preparation; DTL, NTT, TVC: Validation, investigation, Supervision. All authors read and approved the final manuscript.
Funding
None.
Availability of data and materials
Data and materials used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics approval and consent to participate
This study received permission from the Ethics Committee of Hanoi Medical University (decision number: 4397/QD-DHYHN), complies with the ethical standards set forth in the Declaration of Helsinki, and was revised by the World Medical Association’s General Assembly in Seoul, South Korea, in October 2008.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
References
-
Nagtegaal
I.,
Odze
R.,
Klimstra
D.,
Paradis
V.,
Rugge
M.,
Schirmacher
P.,
The 2019 WHO classification of tumours of the digestive system. Histopathology.
2020;
76
(2)
:
182-8
.
View Article Google Scholar -
Kinami
S.,
Saito
H.,
Takamura
H.,
Significance of Lymph Node Metastasis in the Treatment of Gastric Cancer and Current Challenges in Determining the Extent of Metastasis. Frontiers in Oncology.
2022;
11
:
1-14
.
View Article Google Scholar -
Sano
T.,
Kobori
O.,
Muto
T.,
Lymph node metastasis from early gastric cancer: endoscopic resection of tumour. British Journal of Surgery.
1992;
79
(3)
:
241-4
.
View Article Google Scholar -
Tanaka
M.,
Ono
H.,
Takizawa
N.,
Kohei
H.,
Endoscopic Submucosal Dissection of Early Gastric Cancer. Digestion.
2008;
77
(1)
:
23-8
.
View Article Google Scholar -
Sung
H.,
Ferlay
J.,
Siegel
R.L.,
Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA: a cancer journal for clinicians.
2021;
71
(3)
:
209-49
.
View Article PubMed Google Scholar -
Liang
F.,
Cao
W.,
Wang
Y.,
Li
L.,
Zhang
G.,
Wang
Z.,
The prognostic value of tumor budding in invasive breast cancer. Pathology, Research and Practice.
2013;
5
(209)
:
269-75
.
View Article Google Scholar -
Hwang
S.W.,
Lee
D.H.,
Lee
S.H.,
Preoperative staging of gastric cancer by endoscopic ultrasonography and multidetector-row computed tomography. Journal of gastroenterology and hepatology.
2010;
25
(3)
:
512-8
.
View Article Google Scholar -
de Nucci
G.,
Gabbani
T.,
Impellizzeri
G.,
Deiana
S.,
Biancheri
P.,
Ottaviani
L.,
Linear EUS Accuracy in Preoperative Staging of Gastric Cancer: A Retrospective Multicenter Study. Diagnostics (Basel).
2023;
13
(11)
:
2-10
.
View Article Google Scholar -
Anand
D.,
Barroeta
J.E.,
Gupta
P.K.,
Kochman
M.,
Baloch
Z.,
Endoscopic ultrasound guided fine needle aspiration of non-pancreatic lesions: an institutional experience. Journal of Clinical Pathology.
2007;
60
(11)
:
1254-62
.
View Article Google Scholar -
Renzulli
M.,
Clemente
A.,
Spinelli
D.,
Ierardi
A.M.,
Marasco
G.,
Farina
D.,
Gastric cancer staging: is it time for magnetic resonance imaging?. Cancers (Basel).
2020;
6
(12)
:
1-11
.
View Article Google Scholar -
Lugli
A.,
Kirsch
R.,
Ajioka
Y.,
Recommendations for reporting tumor budding in colorectal cancer based on the International Tumor Budding Consensus Conference (ITBCC) 2016. Modern pathology.
2016;
30
(9)
:
1299-311
.
View Article Google Scholar -
Lino-Silva
L.S.,
Salcedo-Hernández
R.A.,
Gamboa-Domínguez
A.,
Tumour budding in rectal cancer. A comprehensive review. Contemporary Oncology (Poznan, Poland).
2018;
2
(22)
:
61-74
.
View Article Google Scholar -
Setoyama
T.,
Natsugoe
S.,
Okumura
H.,
Number of Lymph Node Metastases and Its Prognostic Significance in Early Gastric Cancer: A Multicenter Italian Study. Journal of Surgical Oncology.
2006;
94
(4)
:
275-80
.
View Article Google Scholar -
Li
C.,
Wang
J.,
Kong
J.,
Tang
J.,
Wu
Y.,
Xu
E.,
GDF15 promotes EMT and metastasis in colorectal cancer. Oncotarget.
2016;
7
(1)
:
860-72
.
View Article Google Scholar -
Tsoukalas
N.,
Aravantinou-Fatorou
E.,
Tolia
M.,
Epithelial-mesenchymal transition in non small-cell lung cancer. Anticancer Research.
2017;
37
(4)
:
1773-8
.
View Article Google Scholar -
Querzoli
P.,
Coradini
D.,
Pedriali
M.,
Boracchi
P.,
Ambrogi
F.,
Raimondi
E.,
An immunohistochemically positive E-cadherin status is not always predictive for a good prognosis in human breast cancer. British Journal of Cancer.
2010;
103
(12)
:
1835-9
.
View Article Google Scholar -
Kong
S.H.,
Yoo
M.W.,
Kim
J.W.,
Lee
H.J.,
Kim
W.H.,
Lee
K.U.,
Validation of limited lymphadenectomy for lower-third gastric cancer based on depth of tumour invasion. British Journal of Surgery.
2011;
1
(98)
:
65-72
.
View Article Google Scholar -
de Jong
M.H.,
Gisbertz
S.S.,
Henegouwen
M.I.,
Draaisma
W.A.,
Lymph node metastases rate of locoregional and non-locoregional lymph node stations in gastric cancer. Journal of Gastrointestinal Oncology.
2022;
13
(4)
:
1605-15
.
View Article Google Scholar -
Zuoi
C.H.,
Xie
H.,
Liu
J.,
Characterization of lymph node metastasis and its clinical significance in the surgical treatment of gastric cancer. Molecular and Clinical Oncology.
2014;
5
(2)
:
821-6
.
View Article Google Scholar -
Valastyan
S.,
Weinberg
R.A.,
Tumor Metastasis: Molecular Insights and Evolving Paradigms. Cell.
2011;
2
(147)
:
275-92
.
View Article Google Scholar -
Tian
L.,
Shen
D.,
Li
X.,
Shan
X.,
Wang
X.,
Yan
Q.,
Ginsenoside Rg3 inhibits epithelial-mesenchymal transition (EMT) and invasion of lung cancer by down-regulating FUT4. Oncotarget.
2016;
7
(2)
:
1619-32
.
View Article Google Scholar -
Zlobec
I.,
Lugli
A.,
Epithelial mesenchymal transition and tumor budding in aggressive colorectal cancer: tumor budding as oncotarget. Oncotarget.
2010;
1
(7)
:
651-61
.
View Article Google Scholar -
Bronsert
P.,
Enderle-Ammour
K.,
Bader
M.,
Timme
S.,
Kuehs
M.,
Csanadi
A.,
Cancer cell invasion and EMT marker expression - a three-dimensional study of the human cancer-host interface. The Journal of Pathology.
2014;
234
(3)
:
410-22
.
View Article Google Scholar -
Mendonsa
A.,
Na
T.Y.,
Barry
M.,
Gumbiner. E-cadherin in Contact Inhibition and Cancer. Oncogene.
2018;
37
(35)
:
4769-80
.
View Article Google Scholar -
Gall
T.M.,
Frampton
A.E.,
Gene of the month: E-cadherin (CDH1). Journal of Clinical Pathology.
2013;
66
(11)
:
928-32
.
View Article Google Scholar -
Biswas
K.H.,
Molecular Mobility-Mediated Regulation of E-Cadherin Adhesion. Trends in Biochemical Sciences.
2019;
1
:
1-11
.
View Article Google Scholar -
Bruner
H.C.,
Derksen
P.W.,
Loss of E-Cadherin-Dependent Cell–Cell Adhesion and the Development and Progression of Cancer. Cold Spring Harbor perspectives in biology.
;
10
(3)
:
a029330
.
View Article Google Scholar -
Na
T.Y.,
Schecterson
L.,
Mendonsa
A.M.,
Barry
M.,
Gumbiner. The functional activity of E-cadherin controls tumor cell metastasis at multiple steps. Proceedings of the National Academy of Sciences of the United States of America.
2020;
117
(11)
:
5931-7
.
View Article Google Scholar -
Piccolo
G.,
Zanghi
A.,
Vita
M. Di,
Bisagni
P.,
Lecchi
F.,
Cavallaro
A.,
The role of E-cadherin expression in the treatment of western undifferentiated early gastric cancer: can a biological factor predict lymph node metastasis?. PLoS One.
2020;
15
(4)
:
e0232429
.
View Article Google Scholar -
Torabizadeh
Z.,
Nosrati
A.,
Saravi
S.N.,
Charati
J.Y.,
Janbabai
G.,
Evaluation of E-cadherin Expression in Gastric Cancer and Its Correlation with Clinicopathologic Parameters. Int J Hematol Stem Cell Res..
2017;
2
(11)
:
158-63
.
-
Wu
Z.Y.,
Zhan
W.H.,
Li
J.H.,
Expression of E-cadherin in gastric carcinoma and its correlation with lymph node micrometastasis. World Journal of Gastroenterology.
2005;
11
(20)
:
3139-43
.
View Article Google Scholar -
Grady
W.M.,
Willis
J.,
Guilford
P.J.,
Dunbier
A.K.,
Toro
T.T.,
Lynch
H.,
Methylation of the CDH1 promoter as the second genetic hit in hereditary diffuse gastric cancer. Nature Genetics.
2000;
26
(1)
:
16-7
.
View Article Google Scholar -
Aban
C.E.,
Lombardi
A.,
Neiman
G.,
Biani
M.C.,
La Greca
A.,
Waisman
A.,
Downregulation of E-cadherin in pluripotent stem cells triggers partial EMT. Scientific Reports.
2021;
11
(1)
:
1-11
.
View Article Google Scholar -
Chan
A.O.,
Lam
S.K.,
Wong
B.C.,
Promoter methylation of E-cadherin gene in gastric mucosa associated with Helicobacter pylori infection and in gastric cancer. Gut.
2003;
52
(4)
:
502-6
.
View Article Google Scholar -
Birchmeier
W.,
E-cadherin as a tumor (invasion) suppressor gene. BioEssays.
1995;
17
(2)
:
97-9
.
View Article Google Scholar -
Shimada
S.,
Akiyama
Y.,
Mogushi
K.,
Ishigami-Yuasa
M.,
Kagechika
H.,
Nagasaki
H.,
Identification of selective inhibitors for diffuse-type gastric cancer cells by screening of annotated compounds in preclinical models. British Journal of Cancer.
2018;
118
(7)
:
972-84
.
View Article Google Scholar -
Machado
J.C.,
Oliveira
C.,
Carvalho
R.,
Soares
P.,
Berx
G.,
Caldas
C.,
E-cadherin gene (CDH1) promoter methylation as the second hit in sporadic diffuse gastric carcinoma. Oncogene.
2001;
20
(12)
:
1525-8
.
View Article Google Scholar -
Oliveira
C.,
De Bruin
J.,
Nabais
S.,
Ligtenberg
M.,
Moutinho
C.,
Nagengast
F.M.,
Intragenic deletion of CDH1 as the inactivating mechanism of the wild-type allele in an HDGC tumour. Oncogene.
2004;
23
(12)
:
2236-40
.
View Article Google Scholar -
Kalluri
R.,
Weinberg
R.A.,
The basics of epithelial-mesenchymal transition. The Journal of Clinical Investigation.
2009;
119
(6)
:
1420-8
.
View Article Google Scholar -
Ueno
H.,
Shinto
E.,
Kajiwara
Y.,
Fukazawa
S.,
Shimazaki
H.,
Yamamoto
J.,
Prognostic impact of histological categorisation of epithelial-mesenchymal transition in colorectal cancer. British Journal of Cancer.
2014;
111
(11)
:
2082-90
.
View Article Google Scholar -
Zlobec
I.,
Lugli
A.,
Epithelial mesenchymal transition and tumor budding in aggressive colorectal cancer: tumor budding as oncotarget. Oncotarget.
2010;
1
(7)
:
651-61
.
View Article Google Scholar -
Roh
M.S.,
Lee
J.I.,
Choi
P.J.,
Tumor budding as a useful prognostic marker in esophageal squamous cell carcinoma. Diseases of the Esophagus.
2004;
17
(4)
:
333-7
.
View Article Google Scholar -
Gujam
F.,
McMillan
D.,
Mohammed
Z.,
Edwards
J.,
Going
J.J.,
The relationship between tumour budding, the tumour microenvironment and survival in patients with invasive ductal breast cancer. British Journal of Cancer.
2015;
113
(7)
:
1066-74
.
View Article Google Scholar -
Yamaguchi
Y.,
Ishii
G.,
Kojima
M.,
Yoh
K.,
Otsuka
H.,
Otaki
Y.,
Histopathologic features of the tumor budding in adenocarcinoma of the lung: tumor budding as an index to predict the potential aggressiveness. Journal of Thoracic Oncology.
2010;
5
(9)
:
1361-8
.
View Article Google Scholar -
Zhu
T.,
Hu
X.,
Wei
P.,
Shan
G.,
Molecular background of the regional lymph node metastasis of gastric cancer. Oncology Letters.
2018;
15
(3)
:
3409-14
.
View Article Google Scholar
Comments
Article Details
Volume & Issue : Vol 11 No 9 (2024)
Page No.: 6753-6763
Published on: 2024-09-30
Citations
Copyrights & License
This work is licensed under a Creative Commons Attribution 4.0 International License.
Search Panel
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Search for this article in:
Google Scholar
Researchgate
- HTML viewed - 1695 times
- PDF downloaded - 570 times
- XML downloaded - 72 times
